
Introduction
COVID-19 is challenging health systems globally, and in the UK, the pandemic has triggered an unprecedented research response. Across the UK, teams are designing and delivering studies across a range of COVID research encompassing epidemiology, disease surveillance, disease consequences, early and late phase clinical trials. Early evidence suggests that some segments of the population are at high risk either of contracting COVID or of more severe consequences of COVID including hospitalisation and death. Some of these groups are not well reached by standard research design and delivery mechanisms, and there is growing concern that some of the groups most vulnerable to the impact of COVID are under-represented in research studies.
This guidance is designed to facilitate best practice in the design, funding, approval, regulation and delivery of research on COVID-19 and is a product of the ongoing NIHR INCLUDE project that seeks to improve research for under-served groups.
What is an under-served group?
There is no single definition of an under-served group in research; the definition is context-dependent and will vary depending on the population, disease and intervention being studied. However if a group is enrolled in a study at lower rates than one sees in the population affected by the disease, this is evidence that the group is likely to be under-served. Similarly, if groups known to be at risk of a disease are excluded from participation either because of protocol design exclusions, an intervention that is unsuitable for that group, or because research delivery does not enable them to participate in practice, this too is evidence of the group being under-served.
Who is at risk of COVID-19?
Our knowledge of who is more or less likely to be infected by COVID-19 is limited at present. In the general population it is unclear whether certain groups are at higher risk of contracting the infection (as opposed to suffering severe consequences of infection). However, individuals with a high degree of contact with those who are infected, including healthcare workers, retail staff, and other key workers with face-to-face roles are likely to be at high risk. The other groups in which risk appears elevated are patients who spend prolonged periods of time in close proximity to other patients (for example patients attending hospital-based haemodialysis) and those in care homes: emerging evidence suggests that once COVID-19 starts to affect a care home it can spread very rapidly through the care home population of both residents and staff.
Who is at risk of severe consequences of COVID-19?
Emerging data suggest that a number of groups are at higher risk of death or ICU admission from COVID infection. These groups include, but are not limited to:
- Older people (particularly those aged 70 and over)
- People living with obesity
- Men
- People with multimorbidity
- Care home residents and others living with frailty
- Black, Asian and minority ethnic (BAME) groups
- People with immunosuppression, due to medication, systemic illness or malnutrition
What groups may be under-served by healthcare and research systems with respect to COVID-19?
This is also likely to be context-specific, but examples include:
- Older people and others who are self-isolating (who may not be able to access healthcare easily) on government advice
- Those who may not be prioritised for hospital admission or ITU admission on the basis of high frailty scores, due to chronic and relatively stable cognitive or neurological diseases rather than physical frailty
- Those who lack digital literacy or access to digital technologies
- People with cognitive problems and dementia, especially those living alone, who may not be able to understand and/or comply with the symptom reporting and testing needed for diagnosis.
- Socio-economically deprived groups, who are likely to have less resilience to the economic shocks precipitated by COVID
- People without a car or who live in rural areas (who may find it difficult to access testing facilities that require attendees to come in a car
How can under-served groups be more successfully included in COVID research?
The INCLUDE project contains a roadmap outlining the potential points of intervention to improve the inclusion of under-served groups (Fig 1) and a structure that may be helpful in guiding teams considering how to focus their efforts:
Figure 1. The INCLUDE roadmap
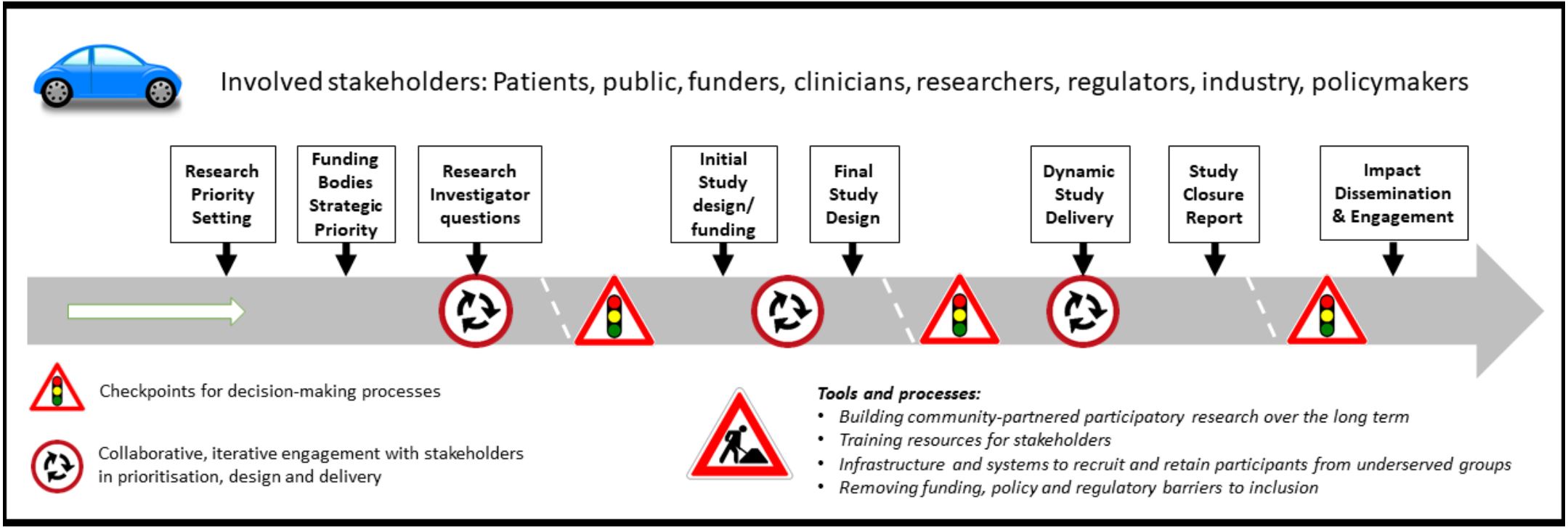
Image - text description
The above road-map diagram lists the stakeholders involved in or affected by outputs from the INCLUDE programme: Patients, public, funders, clinicians, researchers, regulators, industry, policymakers. It also describes the potential points of intervention/processes, in sequential order: Research priority setting; Funding bodies Strategic priority; Research investigator questions; Initial study design/funding; Final study design; Dynamic study delivery; Study closure report; Impact dissemination and engagement. These represent key points for considering inclusion of under-served groups over the life course of the study. Processes are embedded in the context of ethics and regulatory requirements and evolving digital technology developments.
Figure 2. The INCLUDE workstreams
Workstream 1
Communications and training
Workstream 2
Infrastructure, people and processes
Workstream 3
Design tools
Workstream 4
Funder and regulatory landscape
Recommendations and suggestions from the INCLUDE project for COVID research
Research Priority Setting
We recommend that representatives from under-served groups are consulted at the earliest possible time to agree a set of national research priorities for COVID research. A rapid James Lind Alliance project would be one possible way to achieve this, but opportunities also exist to ensure representation on NIHR and UKRI COVID-19 funding committees and prioritisation committees
Funding bodies strategic priorities
We suggest that strategic priorities for research funding bodies (UKRI, NIHR, charities) should reflect the views of under-served groups from any national research priority exercise, as well as reflecting current scientific paradigms and national health and social care system imperatives.
We recommend that PPIE representation should be in place on all COVID-related funding and prioritisation panels and this PPIE representation should encompass representatives from groups who are at risk of being under-served by COVID research.
Research investigator questions
We recommend that research questions should be co-developed by research teams, funders and government, and PPIE representatives including people from under-served groups.
Initial design and funding
We recommend that inclusion criteria are kept to the minimum necessary to ensure patient safety, and that criteria likely to exclude broad sectors of populations are avoided. In particular, we recommend that studies do not overtly or inadvertently exclude participants on the basis of age, sex, ethnicity, geography, socioeconomic status, multimorbidity, cognitive impairment, body mass index or place of residence, unless studies specifically aim to generate data for groups that have to date been under-served by COVID research.
We recommend that interventions are designed and selected to be usable by a wide range of participants, including those from under-served groups. If this is not possible, serious consideration should be given to abandoning the intervention on the grounds that it will not be broadly applicable in practice. Exceptions to this are interventions designed to target a specific biological pathway identified by disease severity or other disease characteristics (i.e. stratified or precision medicine approaches), or interventions designed specifically to target under-served groups where current approaches are not sufficiently effective.
We recommend that outcomes relevant to a broad range of participants are selected, that outcomes should be simple and should place minimal burden on both participants and research teams. Outcomes should be deliverable under pandemic conditions (e.g. when wearing full PPE in overloaded hospitals). Outcomes that can be collected from routinely collected clinical data, or participant-reported outcomes that have the flexibility to be collected by telephone, by video link, by remote devices (e.g. accelerometers or other Bluetooth-enabled devices) or by web-based / SMS interfaces should be preferred
When outcomes must be collected face to face, these should be able to be collected in a range of different environments including the participant’s own home, not just in hospital wards or clinics. Outcomes should where possible be able to be assessed by a range of staff with no or minimal training to ensure that studies are resilient against staff illness or redeployment in future pandemic waves. We suggest that research teams build in the costs of hardware, software and adequate time to support these outcome collection methods into their proposals.
We recommend that researchers design study protocols to allow recruitment through as wide a range of routes as possible. Without good scientific reason, recruitment should not be limited to hospitals, GP surgeries, or care institutions, but should be enabled through all of these routes and others including through community social hubs and organisations, via adverts, web-based signup, verbally over the telephone, in response to SMS and traditional mail, and other routes appropriate to reach particular under-served groups. The emergence of new community networks to support isolated and vulnerable people during the pandemic provides new opportunities for contacting and engaging under-served groups in research.
We recommend that funders apply the checklist given later in this document to assess whether research proposals have been developed in conjunction with under-served groups, and that proposals are designed and will be delivered in a way likely to be able to recruit under-served groups successfully in COVID research.
We recommend that funders ensure that additional funds (above and beyond the amount of money traditionally viewed as adequate to support recruitment and retention) are available to research teams to support successful recruitment of under-served groups. This may require funds for home visiting, transportation (in many cases by car or taxi not public transport), PPE, more screening per participant recruited, longer study visits, provision of translators or translated materials.
Final study design
We suggest that Research Ethics committees pay particular attention to inclusion and exclusion criteria, routes of recruitment, information materials, consent processes (including the needs of those without capacity) and whether under-served groups have been engaged in study design. Where study designs seem likely to fail to include sufficient people from under-served groups, ethics committees should robustly call attention to this, and ask research teams to modify their proposals accordingly even if doing so leads to short delays in approval of projects.
Similarly, we suggest that Sponsor organisations be advised to apply similar scrutiny to research proposals at the design stage and insist on changes where the design makes exclusion of under-served groups likely.
We suggest that Sponsor organisations and research ethics committees should be advised to both welcome and encourage novel and efficient methods of approaching, consenting, recruiting and retaining participants in research studies. Many proposals will be very different from those that organisations are used to seeing, but this should be viewed as an opportunity, not a reason to fall back on traditional (and often ineffective) methods of study conduct.
Study delivery
We recommend that local research delivery teams seek local advice on how to reach and engage with under-served groups. In many cases, this will entail getting advice from members of specific ethnic communities, or those with lived experience of particular population sectors (e.g. those living in care homes, homeless people).
We recommend that training for research delivery staff (local investigators, research nurses and other research team members) be delivered to raise awareness of the need to recruit inclusively, to highlight particular under-served groups, and to provide the generic skills required to engage with specific under-served groups.
We recommend that local research teams configure themselves to be able to recruit in environments other than standard inpatient and outpatient secondary care departments. This should include conducting study procedures in participants’ own homes, care homes, conducting study procedures remotely (e.g. via telephone and video links). Linking with neighbouring healthcare research organisations will enable cross-cover of research staff in the event of staff sickness or of one organisation becoming overloaded by clinical work in future pandemic waves.
We recommend that for trials of medicinal products, dispensing arrangements for oral medications be put in place to enable delivery of medications direct to participants’ homes or local pharmacy rather than a need to collect medication from a research facility. This approach will help to build resilience against future restrictions on movement or closure of workplaces.
We recommend that local research support agencies (such as the NIHR local Clinical Research Networks and NHS Trusts) provide local research teams with the equipment and resources that they need to deliver research in non-traditional settings. This may include transportation, contracts and working practice procedures enabling work in participants’ homes, provision of COVID testing and PPE in line with national guidance, IT hardware and software to enable video links, EConsent and eCRF use whilst roaming, translation services and sufficient time to conduct study visits in non-traditional settings.
We suggest that local research support agencies put in place systems to monitor local recruitment of under-served groups to each study. Combining these local data across studies will enable study teams to adapt their recruitment strategies at an early point, for instance switching place of recruitment, oversampling particular under-served groups, or changing how study teams approach participants.
Study closure and analysis
Investigators and Sponsors should develop plans for how pauses or discontinuation of study activity due to future pandemic waves will be managed (ideally to at least enable study follow up to continue), and how these plans will be communicated to participants.
Study reports and analysis plans should report the proportion of relevant under-served groups and compare these proportions to those found in the general population with COVID-19 illness.
Study analysis plans should include pre-specified subgroups analyses for key under-served groups, both to explore differences within studies, but also to enable later pooling of results from different under-served groups.
Impact, dissemination and engagement
We recommend that all studies devise a comprehensive dissemination and engagement plan, and that representatives from under-served groups should be part of the team drawing up these plans
We suggest that specific engagement plans for different under-served groups should be drawn up to enable appropriate tailoring of messages to different groups, in a way that best encourages feedback, debate and engagement within different groups.
A checklist to guide funders and reviewers in assessing inclusiveness of research
1.Does the topic of the study reflect the priorities elicited by consultation with under-served groups?
2.Have representatives from under-served groups been engaged in the design of the study, and in what way?
3.Does the target population for the study (as defined by the inclusion and exclusion criteria) reflect those who are at risk of contracting COVID or who are at increased risk of the adverse consequences of COVID?
4.Have the investigators taken steps to ensure that these potentially under-served groups will be included in the study with appropriate mitigation of any risks?
5. Are there unnecessary or unjustifiable exclusion criteria (e.g. old age, sex, ethnicity, obesity, cognitive impairment, multimorbidity) or research methods that will act as barriers to inclusion of under-served groups at high risk of COVID infection and its adverse consequences?
6.Is the intervention designed and delivered in a way that is acceptable and feasible to a broad range of people most at risk from COVID infection?
7. Are the study outcomes easy to measure, and can they be measured in a range of different environments? Will they still be able to be measured during the peak of a pandemic wave or during population lockdown?
8. Does the study target a specific under-served group? If so, is adequate justification for this given? In addition, is the strategy proposed to target the group likely to succeed?
A checklist to guide research teams in designing inclusive COVID research
1.Have I engaged with representatives of under-served groups in designing my study question and protocol?
2.Have I avoided inclusion/exclusion criteria likely to lead to exclusion of under-served groups (e.g. age limits, excluding multimorbidities, BMI limits)
3.Is my study intervention suitable for, and acceptable to, under-served groups (e.g. avoiding gelatine capsules on medication)
4.Are my outcomes validated and relevant to a broad range of patients in the populations that my research seeks to serve? (e.g. cognition assessment tools in translated versions)
5.Have I avoided study burden that is likely to make it more difficult for some groups to participate (e.g. frequent study visits)
6.Have I provided a range of recruitment pathways that give flexibility in how participants are sought and contacted (e.g. not confining recruitment to drive-in testing centres, allowing recruitment from care homes)
7.Have I provided study information in a format that is accessible to under-served groups (e.g. translations of study information, simplified study information, information written with a reading age of 9 or below, written in large font size)
8.Have I enabled consent to be obtained in a way that is flexible and tailored to the needs of different groups (e.g. EConsent for those isolating, assent from relatives for those with cognitive impairment). Have I involved carers and assentees in the design of the assent process for studies where consent cannot be obtained from the participant
9.Will my study still be deliverable in the event of a second pandemic wave, with possible increase in lockdown restrictions and study staff redeployment?
A checklist to guide research delivery teams in delivering inclusive COVID research
1.Have we engaged with local representatives from under-served groups to understand how best to approach, recruit and retain participants to this study locally?
2.Are our staff trained to approach and recruit people from under-served groups (e.g. in care homes). If not, what training is required and how will we deliver this?
3.Do our staff have the correct equipment to deliver the study to under-served groups (e.g. portable testing and blood taking kit, car transport and PPE to conduce home visits, contracts and lone working policies to support home working, video and phone consulting systems to enable remote follow up)
4.Do we have staff with particular skills or background who would be well suited to engage with under-served groups (e.g. speak the same language, live in the same area, experience working in a particular healthcare sector)
5.Do we have processes in place locally to monitor whether we are reaching people from under-served groups – and if not, why not?
6.If recruiting people from under-served groups is taking more time or resources, is the extra time and resource being made available, either from the funder or from local CRN resource?
Conclusion
At a time when research on COVID is being designed and delivered at an extraordinary speed, it may seem that the urgency of the situation obviates the need to fully engage under-served groups in the design and delivery of COVID research. We argue however that doing so is not a luxury but a necessity and failure to engage represents an enormous wasted opportunity. It will hamper scientific progress and potentially lead to the deployment of ineffective or harmful diagnostics and therapeutics to large sections of the population. This in turn will lead to worse health outcomes for under-served groups, and healthcare resources being wasted. Fully engaging under-served groups and enabling their inclusion in COVID research is the only way that we will be able to understand the health impacts of COVID in these most vulnerable groups and thus mitigate the impact of COVID on health and society in an equitable way.
Names
- Eleanor Anderson: Specialty Cluster E Project Coordinator, NIHR CRN
- Camille Carroll: National Specialty Lead for DeNDRoN Neurodegenerative Diseases, NIHR CRN
- Paul Dark: Chair in Critical Care Medicine, Manchester University
- Kim Down: Specialty Cluster E Manager, NIHR CRN
- Alistair Hall: Clinical Director, CRN Yorkshire and the Humber
- Helen Hancock: Director, NIHR RDS NENC, Director of the Newcastle CTU
- Joanna Knee: CRNCC RDD Head of Research OperationsEamonn Maher: National Specialty Lead for Genetics, NIHR CRN
- Rebecca Maier: Deputy Lead for Clinical Trials & Engagement, Newcastle University
- Gail Mountain: Professor of Applied Dementia Research, Bradford University
- Gary Nestor: Assistant Specialty Cluster E Lead, NIHR CRN
- John O’Brien: National Specialty Lead for DeNDRoN Dementia NIHR CRN
- Laurie Oliva: Head of PPIE, NIHR CRNCC
- Lynn Rochester (Chair): Specialty Cluster E Lead, Professor of Human Movement Science and Director of Clinical Ageing Research Unit
- James Wason: Professor of Biostatistics, IHS Biostatistics Research Group
- Miles Witham: Professor of Trials for Older People, Newcastle University
References:
- International Severe Acute Respiratory and Emerging Infections Consortium (ISARIC) COVID-19 report April 27th 2020
- Williamson E, Walker AJ, Bhaskaran KJ et al. OpenSAFELY: factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients
- Glasziou PP, Sanders S, Hoffmann T. Waste in COVID-19 research
- Toolkit for increasing participation of Black, Asian and minority ethnic (BAME) groups in health and social care research. December 2018.
National Institute for Health and Care Excellence. NICE guideline 159: COVID-19 rapid guideline: critical care in adults. March 2020.
McMurdo ME, Roberts H, Parker S et al. Improving recruitment of older people to research through good practice. Age Ageing. 2011;40(6):659-65. - The PERSPECTIVES study
Find out more
INCLUDE Ethnicity Framework
The INCLUDE Ethnicity Framework is a tool that helps trial teams think carefully about which ethnic groups should be included in their trial, and what challenges there may be to making this possible. The site also has some examples of how to use the Framework along with other resources linked to involving different ethnic groups in trials.
Journal articles
From BMJ Open
"Ensuring that COVID-19 research is inclusive: guidance from the NIHR INCLUDE project"
From Trials
Citations
For the INCLUDE Guidance (General)
To cite this report: NIHR (2020) Improving inclusion of under-served groups in clinical research: Guidance from the NIHR INCLUDE project. UK: NIHR. Available at: www.nihr.ac.uk/documents/improving-inclusion-of-under-served-groups-in-clinical-research-guidance-from-include-project/25435 (date link accessed)
For the INCLUDE Guidance (COVID-19 specific)
To cite this report: NIHR (2020) Ensuring that COVID-19 Research is Inclusive: Guidance from the NIHR CRN INCLUDE project. UK: NIHR. Available at: www.nihr.ac.uk/documents/ensuring-that-covid-19-research-is-inclusive-guidance-from-the-nihr-crn-include-project/32647 (date link accessed)