
Introduction
In 2015, the NIHR Global Health Research Portfolio was established to support applied health research for the direct and primary benefit of people in low-and middle-income countries (LMICs) on the Organisation for Economic Co-operation and Development (OECD) Development Assistance Committee (DAC) list, using UK Aid from the UK government.
The Global Health Research portfolio is underpinned by three principles which guide development and delivery. These are:
- Meet eligibility criteria as Official Development Assistance (ODA), i.e. funded research directly and primarily benefits people in ODA-eligible countries on the OECD DAC list.
- Deliver high-quality applied health research, building on the Principles of the NIHR: Impact, Excellence, Effectiveness, Inclusion, Collaboration.
- Strengthen research capability and training through equitable partnerships.
The NIHR has established a substantial portfolio of applied global health research and training in areas that are underfunded or where there is an unmet need. The portfolio is delivered through a mix of researcher-led and commissioned calls, many of which fund initiatives to develop and advance global health research career pathways both in LMICs and in the UK, and through partnerships with other major global health research funders.
The intended long-term impact of the NIHR’s Global Health Research portfolio is to contribute to improved health and wellbeing and economic development in LMICs, in support of globally agreed Sustainable Development Goals (SDGs). The Global Health Research Theory of Change sets out how the different activities across the portfolio are expected to contribute over time to improved health outcomes, strengthened health systems and the long-term sustainable growth of the LMIC research ecosystem.
Background / About the NIHR Global Health Research Centres Programme
Investment in research capacity strengthening (RCS) in LMICs supports the development of the human capital required to drive locally appropriate health improvements and to promote social and economic development. NIHR recognises that there is no single agreed definition of research capacity strengthening, but highlights the UK Collaborative on Development Research (UKCDR)’s definition as ‘Enhancing the ability and resources of individuals, institutions, and/or systems to undertake, communicate, and/or use high quality research efficiently, effectively, and sustainably’.
LMIC-led research which responds to local population needs is vital in the context of current and future global health challenges to improve health outcomes and reduce health inequalities. LMIC institutions and researchers are best placed to develop context-relevant and effective solutions and to engage with local communities and policymakers to inform policy and practice. However, RCS opportunities and resources to support this are often limited, particularly in low-resource settings. For example, countries in the WHO Africa region have demonstrated varied progress against RCS indicators for health in recent years, with the least progress seen in the lowest-income countries. There is therefore a need to ensure that new investment not only strengthens existing LMIC research capacity but also enables smaller or less-research intensive institutions to expand their research capability and to move into new areas of research in support of national or regional health and research strategies.
At an institutional level, investment in LMIC research leadership and career development opportunities is expected to support sustained development of a thriving research ecosystem. At a systems level, strengthened capability for dissemination and stakeholder engagement and involvement will also support knowledge exchange and increase uptake of research evidence in policy and practice.
Research capacity strengthening is already the primary focus of a number activities within the NIHR Global Health Research, including NIHR Global Research Professorships, NIHR-Wellcome International Training Fellowships and support to early career researchers through the Royal Society of Tropical Medicine and Hygiene (RSTMH) Small Grants Programme, and TDR (the Special Programme for Research and Training in Tropical Diseases)’s ‘Antimicrobial Resistance Structured Operational Research and Training Initiative’ (AMR SORT IT). In addition, RCS is embedded within NIHR-delivered programmes through support for academic training posts and research support posts. The Financial Assurance Fund (FAF) was specifically created to support institutional financial management capability for existing Global Health Research Units and Global Health Research Groups. Furthermore, in support of wider institutional capacity strengthening, NIHR has contributed to developing the Global Grants Community’s international standards for Good Financial Grants Practice (GFGP), to increase capacity for financial and research management.
The NIHR Global Health Research Centres programme represents a new funding model for NIHR. It has been developed following consultation with existing award-holders, LMIC stakeholders and other funders to respond to gaps and priorities in health research capacity strengthening at individual, institution and systems levels.
The programme supports the ambition of the NIHR Global Health Research portfolio to support the sustainable growth of the wider LMIC research ecosystem and shift its centre of gravity to LMIC-led research. In support of SDG 3 and SDG 17.6, the investment aims to scale up LMIC research capacity and capability through institutional-level research partnerships.
The Centres will address a targeted thematic area in which a need for coordinated, high-quality research and RCS in LMICs has been clearly identified. Importantly, equal value is given to research capacity strengthening as to the production of high-quality research.
Aim and objectives of the Global Health Research Centres scheme
Aim: NIHR Global Health Research Centres will provide a sustainable platform for high-quality applied health research in LMIC institutions to address local needs and improve health outcomes in response to the growing global burden of disease.
Objectives: To achieve the above aim, the NIHR Global Health Research Centres programme will:
- Strengthen LMIC institutional capacity to undertake, manage and disseminate high-quality applied health research
- Strengthen research career pathways across partner institutions
- Engage with local and national stakeholders to develop priorities and increase research uptake to inform policy and practice
- Deliver high-quality research to increase the global evidence base in a targeted thematic area.
Global Health Research Centres are defined as an institution-level consortium which consists of:
- An LMIC Director supported by a UK Co-Director/Deputy Director, both research leaders in their field
- Two research-intensive institutions (at which the LMIC Director and UK Co-Director/Deputy Director are based) with substantial critical mass of existing expertise and underpinning capacity to support high-quality applied research
- Up to three less research-intensive Co-applicant LMIC institutions, at which the Co-applicant researchers/Principal Investigators are based
- A relevant, coherent and sustainable programme which is jointly developed and delivered to strengthen LMIC research capacity and capability and produce high-quality outputs within the priority area of research.
Each Centre will self-determine its leadership model, structure and research objectives as appropriate to locally-identified research capacity strengthening priorities and clinical, community and policy needs in the priority area.
Thematic research priorities / focus of the call
As defined by the Global Alliance for Chronic Diseases (GACD), Non Communicable Diseases (NCDs) are diseases that are not passed directly from person to person and are of long duration and generally of slow progression. There are a wide range of NCDs, including musculoskeletal disorders, neurological diseases, and many more. However, the five main types of NCDs globally are cardiovascular diseases (e.g. heart attacks and stroke), certain cancers, chronic respiratory diseases (e.g. chronic obstructive pulmonary disease and asthma), diabetes, and mental disorders.
The growing global burden of NCDs is recognised in SDG 3.4, which aims to reduce premature mortality from NCDs by one third by 2030 through prevention and treatment, and by promoting mental health and well-being. However, World Health Organisation (WHO) reports show that prevalence is growing. In 2013, the Global Action Plan for the Prevention and Control of NCDs 2013-2020 confirmed that 36 million people die from NCDs each year (63% of global deaths), including 14 million people under 70 years of age. By 2019, the WHO’s Independent High-level Commission on noncommunicable diseases reported that global NCD-related deaths had increased to 41 million people per year, including 15 million under 70 years of age. More than 80% of these premature deaths from NCDs occur in LMICs, and this figure is expected to continue to increase.
Objective 5 of the WHO Global Action Plan on NCDs also highlights the need for multidisciplinary research:
“Although effective interventions exist for the prevention and control of NCDs, their implementation is inadequate worldwide. Comparative, applied and operational research, integrating both social and biomedical sciences, is required to scale up and maximise the impact of existing interventions”.
In addition, given the nature of NCDs, their causes and consequences depend on local cultural, social, economic and political contexts, there is a strong need to have local capacity to conduct contextually relevant NCD research to inform policy and practice in LMICs. Generating cost-effective interventions for NCDs in LMICs would then help to reduce the evidence-implementation gap.
The NIHR Global Health Research portfolio has already developed a significant and diverse portfolio of NCD research, including multimorbidity and mental health, through programmes which are directly funded through the NIHR, as well as through partnerships with other funders.
Recognising the growing burden and complexity of NCDs in LMICs, the ambition of this call is to develop a critical mass of sustainable applied health research capacity at local level and increase the number of internationally competitive LMIC researchers and research institutions in this field.
The NIHR is therefore seeking applications for Global Health Research Centres that will support RCS across participating LMIC institutions to aid the delivery of high-quality applied health research in NCDs and provide a platform for sustainable growth of the LMIC research ecosystem.
NIHR is seeking Global Health Research Centre applications that take an interdisciplinary approach across participating institutions to address research in the following areas:
- Institutional research plans that focus on NCDs in LMIC populations, at any stage(s) across the lifespan (i.e. from pregnancy/foetal development through childhood and adolescence to all stages of adulthood – including aging adults)
- Drive innovation in the development and evaluation of cost-effective, context-relevant interventions and strategies to improve the primary and secondary prevention, treatment, management and care of NCDs and multiple long-term conditions in LMICs, which could increase the global evidence base through research on (but not limited to):
- Interventions to prevent NCDs in LMICs – focusing on more than one NCD across partner institutions.
- Interventions to improve screening, diagnosis, treatment, management (or lifestyle modification plans) and care of patients with NCDs prevalent in LMICs.
- Interventions for the prevention of the development, and treatment, of NCDs in children and young adults, driven by malnutrition and/or poverty.
- Scalable treatment and care approaches that integrate the management of NCDs with other diseases and multiple long-term conditions/co-morbidities (including infectious / communicable diseases and mental health), in LMICs.
- New NCD treatment packages, or new models of care and community-based interventions that integrate both social and biomedical sciences, in order to scale up and maximise the impact of existing interventions.
- Research to strengthen healthcare systems and delivery models in low resource settings and increase health equity in LMICs, for improved diagnosis, treatment, management and care for those affected by NCDs.
Global Health Research Centres - Theory of change
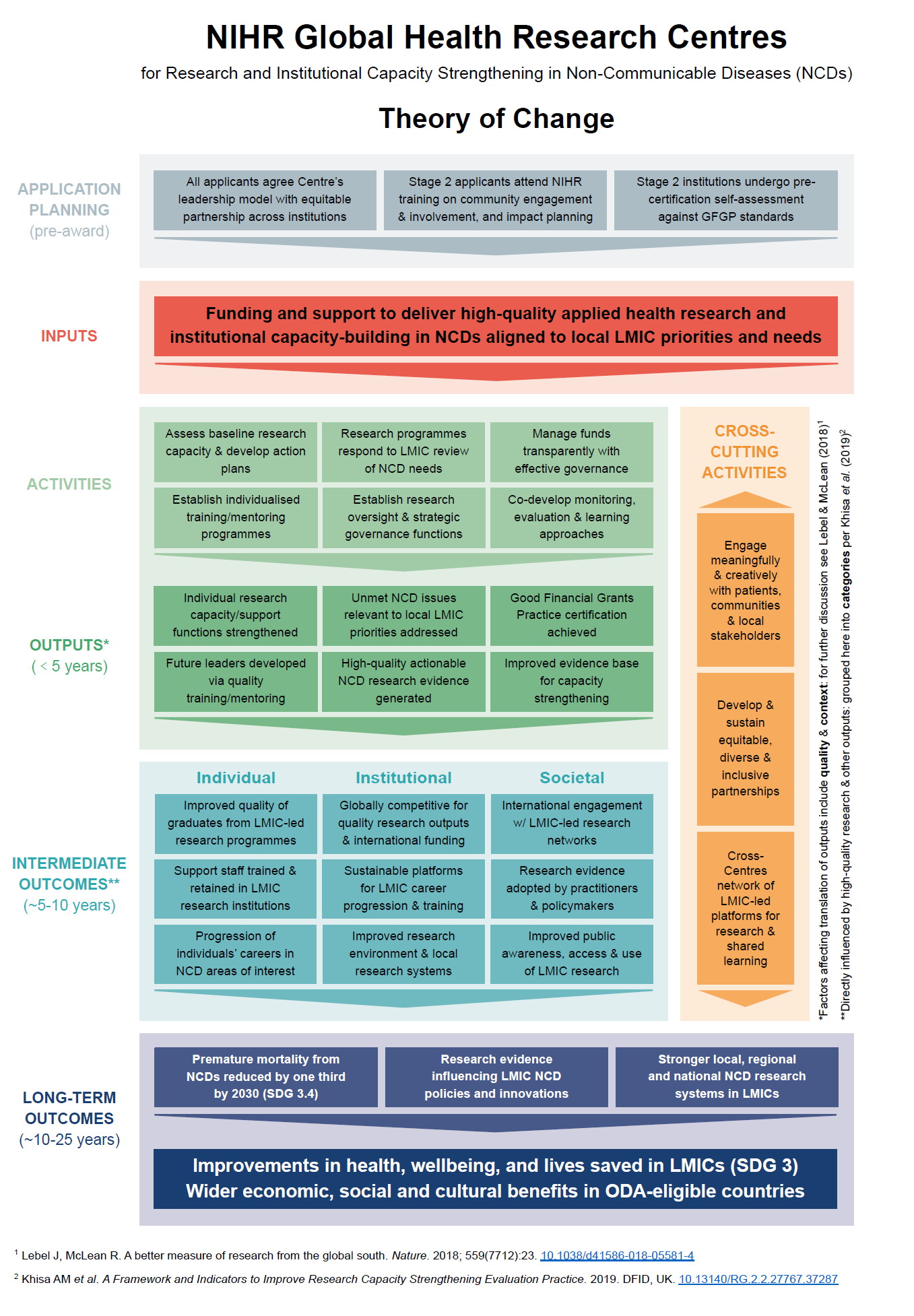
NIHR has developed this Theory of Change to illustrate to potential applicants to the NIHR Global Health Research Centres call a selection of example activities, outputs, and outcomes reflecting the Centres’ core aims, objectives, and funding criteria. We would emphasise that it is intended merely as a visual representation of the Centres core principles and ambitions, drawing on scoping work and discussions that have informed the Centres initial commissioning. Thus we would encourage applicants to think creatively and broadly in how they interpret and further build on the Theory of Change, in terms of how concepts apply in their own local contexts.
NIHR intends and expects this Theory of Change to be updated and evolve as part of activities linked to successful Centres’ own strategies to deliver wider impacts, and monitoring, learning and evaluation plans - and welcomes prospective applicants’ feedback on how the principles and ambitions set out in this guidance relate to their own ambitions, contexts and experiences. Please email ghrcentres@nihr.ac.uk with any feedback.
Budget / Length of funding
NIHR anticipates funding a limited number of Global Health Research Centres, with awards of up to £10 million per Centre over five years. The amount to be requested for the funding period should be fully justified according to Centre applicants’ proposed NCD research and RCS needs in the ODA-eligible countries, given that both are equally essential components of this Call.
Individual Centres may have the possibility to extend their funding for an additional two years, subject to funding and resource availability, as well as the successful completion of NIHR’s mid-contract review.
Applicants should refer to the Global Health Research Centres Finance Guidance for full detail of eligible costs and other budget/finance-related information for this Global Health Research Centres Call. However, specific, reasonable costs that Centre applicants are eligible to apply for are provided below:
- Costs associated with developing a suitable research environment in LMIC partner institutions to enable the effective delivery of the planned research and RCS activities
- Costs associated with formal certification for Good Financial Grants Practice (GFGP) (if successful at Stage 2)
- A ringfenced fund to support career development through a variety of internal, competitive opportunities eg. completion of training modules, researcher exchange or enabling early career researchers to lead on work packages
- Costs associated with the monitoring, evaluation and learning (MEL) of the Centre’s progress against its stated objectives
Note: In the request for funding, it is important for applicants to reflect on and provide appropriate justification for the proportion or percentage split of NIHR funds:
- between UK and LMIC institutions
- between NCD research intensive and lesser experienced LMIC institutions
The flow of funds should ideally reflect where the research is to be conducted and how this will support the RCS objectives of the call.
Scope
Key criteria for funding
The NIHR Global Health Research Centres programme will provide funding to ambitious, transformative, innovative and collaborative consortia that treat high-quality NCD research, and research capacity strengthening in the LMIC institutions as equally essential components.
The following key criteria for the Call encompass the overarching NIHR principles and contribute towards the aims of the GHR portfolio as a whole. These key criteria for funding are incorporated within the Funding Committee’s Selection Criteria, which will be used to assess applications at Stage 1 and 2.
Applications for Global Health Research Centres will be required to describe how they address the following key criteria for funding:
- Research Capacity Strengthening: Institutional commitment to the development of a strong NCD research culture and environment within and across all participating institutions, and in particular the Co-applicant institutions, should be demonstrated by clear identification of institutional capacity strengthening needs, and plans to build, strengthen and expand NCD research and /or training through investment at the institutional level, including by supporting early career NCD researchers (e.g. masters, PhD and postdoctoral). The role of Joint Lead Institutions in supporting this should be clear. Applications should outline plans to develop or strengthen the capacity and capability of research-enabling functions (e.g. in finance, programme and research management) through appropriate recruitment and training opportunities to enhance individual professional development and institutional processes,as well as strengthening systems of evidence use to support dissemination and inform policy and practice.
- Research Excellence: It is expected that Research Excellence will be demonstrated through:
- Quality of the research design and work plan (i.e. clear NCD research questions/objectives, sound design and detailed methodology to address the questions and meet the objectives; clear milestones, identification of possible risks and factoring in ethical considerations).
- Strength of the institutional-level consortium’s research in the chosen NCD (i.e. depth and breadth of relevant NCD research leadership and expertise, and track record of Joint Lead Applicants). This will be balanced with the need for capacity strengthening in the LMIC Co-applicant Institution(s) now venturing into, or that are less experienced in, clearly identified area/s of NCD research, and the plans developed by the Centre for achieving success.
- Applicants should demonstrate that the planned NCD research is robust, enables the development of individuals and institutions to produce high-quality scientific research evidence and interventions, with the intention of strengthening the local, national and regional environment and systems for conducting internationally competitive health research relevant to LMIC contexts. In addition, applicants should outline activities which promote interdisciplinary approaches to working by including expertise / activities associated with a broad range of disciplines such as clinical, health economics, statistics and social sciences.
- Relevance: Applications should demonstrate that the proposed research and RCS fills a significant gap, addresses unmet NCD needs and priorities in ODA-eligible countries and aligns fully with the scope of this call. The Centre’s research plans should be based on an LMIC-led review of the local needs as related to NCDs that is rooted in existing research literature and health system(s), and has refined relevant research questions and priorities through knowledge generation and exchange and engagement with policy makers, evidence users and local communities.
- Leadership: The Centre’s chosen leadership model and the respective roles and responsibilities of both Joint Lead Applicants are clearly defined and agreed. Evidence should be provided that both the LMIC and UK Joint Lead Applicants, and the institutions they represent, have substantial, high-quality expertise in the chosen NCD research theme and are committed and able to support training and capacity development of partner LMIC institutions that have less or no experience in this area of research, if funded.
- Equity and Equitable Partnerships: The proposed research plans outlined should build or strengthen equitable research partnership and boost collaboration across a network of universities and research institutes in LMICs and the UK that wish to tackle the challenges of NCDs in LMICs. Promotion of equality, diversity and inclusion and collaboration, are expected to be strongly reflected in all aspects of the Centre. Also, evidence should be provided regarding how each institution within the consortium will contribute to achieving the Centre’s shared NCD vision and ambition, as well as how they will each benefit directly by participating in the Centre. It is expected that equity will be embedded within the research cultures of all participating institutions.
- Governance: Applications should include appropriate and high-quality plans for effective programme management, governance and contract management. This should incorporate a clear definition of roles, risk management arrangements, including external oversight, and how the efforts of individuals and institutional members will be coordinated. Clear justification for the structure (e.g. institutional composition) and location of the Centre, and how this will support aims and objectives for advancing research in the chosen NCDs, should be provided.
- Stakeholder and Community Engagement and Involvement: There is evidence of active engagement with research participants and the general public within a given community, especially vulnerable groups who are at the greatest risk, as well as other relevant and appropriate local stakeholders (e.g. policy makers and practitioners), throughout all stages of the NCD research and activities.
- Impact and Sustainability: Centres are expected to have a clear and implementable strategy for pathways to impact of the proposed work, in terms of intended NCD health outcomes, and research and capacity strengthening. These should be clearly described in terms of how activities are expected to contribute to wider outcomes (e.g. sustained funding, NCD research uptake by ministries/policy makers, and knowledge exchange - to improve practice and support future sustainability of NCD research in partner LMICs). Plans for meaningful and sustained engagement with communities and the public, practitioners, and policy makers at an early stage and throughout the Centres delivery, should be outlined. Applications should demonstrate a considered and embedded approach to monitoring, evaluation and learning. As part of this, NIHR Global Health Research Centres will be expected to develop their own Theory of Change and frameworks for the evaluation of NCD research and RCS, working in partnership with NIHR to further inform and develop the Centres programme Theory of Change.
- Value for Money: Evidence of a clear, well-justified budget that represents good value for money is required. Applications must demonstrate that all planned expenditure is proportionate and appropriate against the planned activities outlined in the application and consider Economy, Efficiency, Effectiveness and Equity (please see the NIHR GHR Core Guidance for more information on value for money).
Please read the ‘Additional specific guidance for 'NIHR Global Health Research Centres Call' (further below) for more information/suggestions for meeting the key criteria above. For illustrative examples of domains of change and activities that might be included in any pathway to impact, please see Centres Theory of Change as well as Dissemination, Outputs and Anticipated Impact section of this guidance. Also note that the NIHR GHR Core Guidance has other relevant generic information (e.g. CEI, Approach to Risk Management and Assurance, Reporting Requirements).
In scope
NIHR Global Health Research Centre awards will support applications that:
- Demonstrate that they address the published key criteria provided for the Global Health Research Centres Call.
- Propose institutional level applied health research projects/programmes that primarily and directly address the NCD challenges faced by people and patients in ODA-eligible country/ies.
- Incorporate research questions around gender, age, social barriers to health, economic impact and equity that are directly relevant to the LMICs involved in the consortium.
- Include multi-disciplinary and/or interdisciplinary applied health researchers from the UK and LMIC institutions, with relevant expertise and a track-record (for the Joint Lead Institutions) of ensuring research in NCDs is transferred into benefits for patients.
- Demonstrate equity and collaboration in programme leadership, decision-making, capacity strengthening, governance, appropriate distribution of funds, ethics processes, data ownership, and dissemination of findings.
- Include engagement with relevant policy makers and practitioners, patients, the public, civil society organisations, communities and charities.
- Propose a coherent and sustainable plan for capacity and capability strengthening, at all levels and particularly at the institutional level, across Centre institutions.
- Demonstrate the strength of UK / LMIC institutional commitment to the research partnership
- Articulate career development structures for participating LMIC scientists and institutions that outline approaches to develop research leaders across the consortium.
- Provide a convincing long-term vision for the research outcomes, articulating pathways to impact and identifying viable mechanisms for translation in the LMIC context.
Out of scope
NIHR Global Health Research Centres will NOT support applications that:
- Do not meet the published call criteria for Global Health Research Centres.
- Focus solely on NCD research with no substantive focus on RCS or vice versa.
- Only include well-established research institutions.
- Only include limited methodological approaches (e.g. randomised controlled trials, evidence synthesis, service evaluations) or limit their focus to:
- Observational research, secondary research or health policy implementation.
- Basic laboratory/discovery NCD research or experimental medicine
- Replicating research already undertaken in High-Income Countries – Centre research proposals should be clearly relevant to the ODA-eligible country/ies in which the research is to be undertaken
- Conduct research focused on a single NCD.
- Do not consider career development and capacity strengthening for research-enabling functions
- Do not consider the wider research environment
- Do not consider how to strengthen systems of evidence use
Eligibilty
ODA Eligibility
The NIHR Global Health Research portfolio supports high-quality applied health research for the direct and primary benefit of people in low and middle-income countries (LMICs) on the OECD’s DAC list, using Official Development Assistance (ODA) funding.
In order to be eligible to receive NIHR Global Health Research funding, applications must demonstrate how they meet ODA compliance criteria and outline:
- Which country or countries on the OECD DAC list of ODA-eligible countries will directly benefit?
- How the application is directly and primarily relevant to the development challenges of those countries?
- How the outcomes will promote the health and welfare of people in a country or countries on the DAC list?
Where some elements of the research is not undertaken in an ODA-eligible country during the course of the award (including where a country graduates from the DAC list during the lifetime of the award, or there is a need for specialist expertise), the application must clearly state the reasons for this, with due consideration to the benefit of the research to ODA-eligible countries.
Further information can be found at:
- NIHR ODA Guidance for Researchers
- What is ODA
- ODA – definition and coverage
- OECD DAC list of ODA eligible countries
- OECD DAC Statistical Reporting Directives
- OECD Development Co-operation Directorate
Who can apply
All NIHR Global Health Research Centre applications must be led by an LMIC Director (LMIC Joint Lead Applicant) and UK Co-Director/Deputy Director (UK Joint Lead Applicant). There must be two Joint Lead Institutions (one being in an ODA-eligible country and the other in the UK) that have expertise in NCD research. There must also be clear plans to develop a partnership with at least one, and up to three additional Co-applicant LMIC Institutions that aim to build, strengthen or expand their research expertise, capacity and capability in more than one relevant NCD they pre-identify.
The LMIC Joint Lead Institution is the research institution where the Centre Director/LMIC Joint Lead Applicant will be based. They must be legally registered in an ODA-eligible country and will need to be Higher Education Institutions (HEIs) or Research Institute. In addition, these institutions must have a track record of excellence in collaborative research partnerships.
The UK Joint Lead Institution must be legally registered in the UK and would normally be a HEI or Research Institute. Such institutions must also have a track record of excellence in collaborative research partnerships. Funding and contracting for the Centres will take place via the UK Contracting Institutions.
Under this Global Health Research Centres Call, NIHR will only accept a maximum of two applications from a UK or LMIC Joint Lead Institution. Where two applications are submitted from the same institution, each Centre must be distinct in its aims, objectives and geographical area. LMIC Joint Lead Institutions can be Co-applicant Institutions on one other Centre application.
- Joint Lead Applicants: The Joint Lead Applicants will normally be researchers employed at an eligible LMIC or UK based HEI or Research Institute, respectively. They will both have appropriate reputation and standing within their employing organisations, and demonstrable ability to lead and manage a large-scale programme of global health research and RCS focused on NCDs.
Under this Global Health Research Centres Call, an individual cannot be named as a Joint Lead Applicant on more than one application. They can however be a named Co-applicant on one other application and a Collaborator on up to two other Centre applications.
- Co-applicant Institutions: The research institution where the Co-applicant researcher/Principal Investigator is employed. They must be legally registered in an ODA-eligible country and will need to be Higher Education Institutions (HEIs) or Research Institutes.
For each Centre application, there can be up to three Co-applicant Institutions and each of those must be represented by one Co-applicant researcher/ Principal Investigator.
- Collaborators can also be involved in Global Health Research Centre consortia. There will be no limits placed on the number involved, so long as they are necessary to effectively deliver the Centre’s aims and objectives.
Please note: NHS organisations, commercial organisations or governmental agencies cannot be Joint Lead Applicant or Co-applicant Institutions on Global Health Research Centre applications.
For more information about who can be considered as a Co-applicant or Collaborator please refer to Research Expertise / Structure of Team section.
All applicants are strongly encouraged to check eligibility prior to application by e-mailing ghrcentres@nihr.ac.uk.
Selection criteria for Stage 1
The selection criteria for the Global Health Research Centres Call 1 Stage 1 applications will focus on the following four key criteria:
- Research Capacity Strengthening
- Research Excellence
- Relevance
- Leadership
Please refer to the key criteria in Section 6.1 for details of what is expected to be demonstrated in the application for each of these criteria.
Applicants are expected to consider the remaining key criteria (e-i) at Stage 1 to ensure they are embedded in the research strategy throughout proposal development but are not expected to provide much detail at this stage. The remaining key criteria will form part of the selection criteria at Stage 2, therefore applicants who are successful at Stage 1 will be expected to develop their proposal and provide much more detail on the remaining criteria at Stage 2.
Selection criteria for Stage 2
At Stage 2 the selection criteria will be expanded to include all 9 key criteria.
Applicants will be asked to provide detailed plans for CEI, programme management and governance, dissemination and impact and a detailed budget as well as develop their research strategy and RCS plan in line with Stage 1 feedback. The funding committee will be expanded at Stage 2 to include experts to review these aspects of the application in more detail.
Selection process
The NIHR Global Health Research Centres Call is a two-stage competition.
At Stage 1, applicants are expected to submit an outline of the proposed research and RCS plan for review, scoring and shortlisting by an independent international Funding Committee, based on the published eligibility and selection criteria for the Global Health Research Centres Call. The Funding Committee will recommend to the Department of Health and Social Care which applications should be shortlisted to the next stage. Proposals that score below the Funding Committee’s agreed threshold will be rejected at that point and will receive feedback.
At Stage 2, applicants who are successful at Stage 1 will be invited to submit a full application – which will require more detailed information, such as for CEI, and a full financial breakdown. The application will be considered by the Funding Committee and an interview will also be conducted as part of the Stage 2 assessment. The Funding Committee will then recommend to the Department of Health and Social Care which applications should be supported.
Timetable for the Global Health Research Centres call
|
Milestone |
Date |
|---|---|
|
Call launch |
14 October 2020 |
|
Deadline for scope enquiries |
24 March 2021*. |
|
Deadline for receipt of Stage 1 application (via the online NIHR Research Management System [RMS]) |
31 March 2021 1pm UK time |
|
Funding Committee review |
June 2021 |
|
Applicants notified of outcome for Stage 1 |
July 2021 |
|
Stage 2 opens for successful Stage 1 applicants |
July 2021 |
|
Deadline for receipt of Stage 2 application (via the online RMS) |
November 2021 |
|
Funding Committee review |
March 2022 |
|
Applicants notified of outcome for Stage 2 |
April 2022 |
|
Centre starts |
01 September 2022 |
*NIHR will not guarantee to be able to answer queries about the scope or content of applications after this date. If you have other queries about RMS or the application process, please do contact us after this time.
Additional specific guidance for NIHR Global Health Research Centres call
The NIHR Global Health Research Programme Core Guidance covers the key principles supported by all NIHR Global Health Research funding.
The guidance below contains information which is specific to this call. This supports the key criteria and should be read in conjunction with the Core Guidance.
Research expertise / Structure of the team
Global Health Research Centres are required to have both a LMIC and UK Joint Lead Applicant but the approach to joint leadership is intentionally flexible. The LMIC Joint Lead Applicant is expected to fulfil the role of Centre Director, however beyond this the applicants should decide which leadership model best suits their proposed Centre structure. For example applicants may wish to operate a Co-Director model or have a LMIC Director and UK Deputy Director. The chosen approach should be clearly described in the application with an explanation of how this will support the Centre structure and allow the Centre to deliver against its stated aims and objectives.
The number of institutions participating in a Centre consortium is limited to five (please see the eligibility and who can apply sections above for specific definitions for institutional partners). However, the structure of the Centre’s institutional-level research teams, such as which UK institution to include, the ODA-eligible countries or geographic areas, the respective roles of Co-applicant institutions, as well as the number/type of collaborators/service level providers to include in Centre applications have been left flexible by intention. This flexibility is to allow Centres to define and design what is best suited to their specific research questions and RCS plans for the NCDs of interest - as informed by the local and regional needs, so long as they address the key criteria for funding. Therefore, for example, if a Centre has a number of potential institutional partners across a region, then it may be ideal to propose a regional Centre. If the research question and population are concentrated in a single country, then that could be the geographic area.
In their applications, Centres would need to clearly demonstrate how their structure, location and size (including the pool of NCD researchers, resources, early career researchers to be supported and supervisors) are robust enough to achieve their (and the NIHR’s) aims and objectives for advancing research into the NCDs chosen by the Centres themselves, without introducing undue complexity in the management and set up arrangements within the available timeframe. It would also be important to provide evidence that the chosen UK and LMIC Lead Institutions (and their representative Joint Lead Applicants) have strong capability in the NCD thematic area, and the underpinning facilities to perform high-quality research and support RCS in Co-applicant institutions.
Centre consortia are expected to have interdisciplinary expertise that will facilitate institutional partner and stakeholder coordination, training and capacity strengthening in the NCDs of interest, as well as integration of Community Engagement and Involvement (CEI) and Monitoring, Evaluation and Learning (MEL), throughout the Centre’s research programme. As a result, Centres may include as many Collaborators as needed to deliver the research and RCS strategy. Collaborators should be named in the application and their contribution should be clearly described and well justified.
Please note Co-applicants are those individuals with responsibility for the day-to-day management and delivery of the project who form your project team/consortium. Co-Applicants are expected to share responsibility for its successful delivery. Collaborators are those who provide specific expertise on particular aspects of the project and would form part of your wider research team but do not share in the responsibility for the delivery of the project.
Training and Research capacity strengthening
For this Global Health Research Centres Call, applicants will need to provide a clear rationale/plans for developing or strengthening sustainable NCD research capacity and capability in the LMIC institutions. The proposed training and RCS programme should be based on an explicit Theory of Change and understanding of existing gaps and needs of all LMIC institutions in each consortium. This RCS programme should also complement any existing institutional and national research and training strategies, and obtain high-level buy-in. Furthermore, the Global Health Research Centres should consider where programme funded research training and capacity strengthening can be made available to participants from outside the Centre, to maximise impact. Examples of areas for strengthening capacity are provided below but applicants are strongly encouraged to be innovative and creative in developing their own tailor-made Centre training and RCS plans, to meet their consortia’s needs:
- IndividuallevelRCS includes (but is not limited to):
- Support formal training posts (i.e. Masters, PhD, postdoctoral, etc.) with provision of quality supervision. Details must be provided about the planned numbers of each type of post to be provided to nationals of ODA-eligible countries that are involved in the Centre, and how gender parity will be supported.
- Ensure that researchers and research support staff have access to core research training and qualifications in relevant technical skills.
- Ensure provision of training in disciplines such as health economics, statistics and social sciences
- Ensure that provision is made for ‘soft’/personal development skills such as research leadership, grant writing, communication, critical thinking methodologies, etc.
- InstitutionallevelRCS includes (but is not limited to):
- Establish mentorship and supervision systems that are sensitive to culture and gender. Also, maximise the opportunities to share skills within and between Centre institutions, and beyond, by identifying opportunities for strategic networking.
- Curricula development, institutional mentorship, coaching, buddying, exchange and training programmes and workshops, research resources (e.g. library, new training programmes, lab accreditation, etc.).
- Salaried support posts: Global Health Research Centres should target the recruitment, training and retention of roles in areas such as research management, project management, grant management, finance management, data and intellectual property management, information technology, contracting, community engagement and involvement, monitoring, evaluation and learning, knowledge transfer, librarians, technicians, etc. This is important, particularly in the less research intensive institutions (with a focus on NCDs), as such roles are critical for the sustainable delivery and dissemination of research.
- Provide access to appropriate equipment, underpinning facilities, guidance/policies for NCD research, where needed, and train staff to use these.
- Improve processes such as procurement and/or quality control, where relevant.
- Set up and/or participate in forums to share and learn from RCS experiences, challenges and successes.
- Identify opportunities for engagement/Influence in institution-wide strategies/policies.
- Develop an institutional research culture, with the creation of senior leadership roles and research teams, career structures, protected time for NCD research, set up or strengthen research offices, and more. Have a plan for sustaining these beyond the duration of the Centre.
- Societal/Ecosystem/EnvironmentallevelRCS includes (but is not limited to):
- Conduct NCD research that informs national/international policy and has societal benefits/impact, to address SDG3.4.
- Sustained engagement to strengthen systems of evidence use eg. facilitate exchanges or placements with policy-making institutions and practice-based settings.
- Influence national/regional research systems (e.g. funding allocation; productivity trends).
- Establish or participate in international networks/collaborations (e.g. training hubs; international mentorship) to meet SDG17.
- Ensure research uptake and develop dissemination plans.
Given the need to address both excellence and equity as linked, rather than competing considerations for impactful and sustainable research collaborations, NIHR Global Health Research Centre applicants should explain their rationale for allocating training awards in their applications (e.g. whether and why such opportunities are to be spread equitably across partner institutions, or through a competitive recruitment process, or by other means/combinations, bearing in mind gender parity requirements). It is expected that opportunities/activities will take place in the ODA-eligible countries and/or the UK. NIHR Global Health Research Centre applicants will therefore have to decide and justify the approach they use.
Note that in order to maximise the collective impact of the cohort of NIHR Global Health Research Centre consortia, individual training awards (e.g. PhD and postdoctoral researchers) will also become “NIHR Academy Members”, if these training posts are at least 25% funded by the NIHR.
Applicants should also explain how they plan to sustain such institutional-level training, early career research and research-enabling posts/activities beyond the NIHR Global Health Research Centre award, if successful.
Funded NIHR Global Health Research Centres will be expected to have a named Training Lead to coordinate activities across the programme and to join the Centre’s board. Once awards are made, the NIHR will encourage strategic engagement/collaboration by Training Leads and other representatives across different Global Health Research Centres, to enable mutually beneficial learning and knowledge exchange for addressing RCS in NCDs in different contexts within the LMICs.
Applicants should consider the GFGP self-assessment status of Global Health Research Centre institutions (particularly the less-research intensive ones, with respect to chosen NCDs) to ensure appropriately considered training plans are designed and reasonable budgets are included. The budget can include the cost of formal GFGP certification by a Certified Body during the course of their Centre award. This would be detailed in the Stage 2 applications. Such strategic planning towards GFGP certification should facilitate the strengthening of financial processes and management in LMIC institutions that are successful in their Centre applications, which could result in positive and sustainable impact in those institutions.
Applicants may find the following resources useful:
- ESSENCE Seven Principles for Strengthening Research Capacity in Low-and Middle-Income Countries (2014)
- UKCDR Research Capacity Strengthening Tools, Resources and Guides.
Equitable and sustainable partnerships
Partnerships proposed in Centre applications may build on existing relationships or represent the development of a new collaborative relationship. Applications should describe the approach to ensuring equity in partnerships and demonstrate how the partnerships will be able to deliver and sustain their research and capacity strengthening goals in the countries involved.
In line with the International Development (Gender Equality) Act 2014 and the Equalities Act 2010, as well as NIHR principles, NIHR expects equity, diversity and inclusion considerations to be strongly reflected in programme leadership, decision-making, capacity strengthening, governance, appropriate distribution of funds, ethics processes, data ownership, authorship and dissemination of findings. All proposals should consider input from and equitable representation of researchers, for example, from countries involved in the research, of different genders, at all career stages, and from multiple disciplines. There should be no disadvantages relating to areas of diversity, such as gender or disability or any other protected characteristics. As well as being assessed as part of the application process, the approach to equitable partnerships will be monitored and evaluated throughout the lifetime of funding.
Examples of how to achieve the above aims include:
- All parties listed as Joint Lead or Co-applicant within the research team must have significant input to the research and its management (from the co-design stage through to dissemination), and should form an integral part of the leadership structure. Research partnerships should clearly demonstrate gender parity, diversity and inclusion within the leadership, research prioritisation and design, research and capacity building activities and promote mutual benefits for all partners.
- All funded partnerships must have a strong underpinning research ethic based on mutual respect and understanding for different cultural, ethnic, social and economic beliefs and practices.
- The budget should be driven by the complexity and level of ambition for the work plans and partnerships. The NIHR expectation is that funds will be distributed equitably between partners, and that the flow of funds will reflect where the majority of work is taking place and strongly underpin capacity strengthening within LMICs.
- The roles and contributions of all members working as part of the partnership must be clearly stated within the application and reflect meaningful and quality collaborations. Full consideration should be given to additional complexity of managing large collaborations.
- When publishing outputs, lead and senior authors should reflect the full and fair range of contributors across institutions and career stage
- Applicants should consider:
- Will the number of proposed Co-Applicants (and Collaborators) introduce undue complexity in the management and set up arrangements within the available timeframes?
- Will there be sufficient funds available to support all partners to make a meaningful contribution?
- Is the size and breadth of expertise in the team justified and appropriate for delivery of the proposed programme?
Contracting organisations will confirm institutional support through sign-off of the application on electronic submission. In addition, letters of support from the Joint Lead and Co-applicant institutions are a mandatory upload. The letters of support should be from the Vice Chancellor (or equivalent) and describe how the Centre will support the institutions strategy, as well as any staff and resources that will be available to the Centre.
A limited number of letters of support from other major contributors may also be submitted at Stage 2.
You can read further guidance to support developing and sustaining Equitable Research Partnerships. Applicants may find the following resources also useful:
- A Guide for Transboundary Research Partnerships (Swiss Commission for Research Partnerships with Developing Countries (KFPE)
- The UKCDR report on building effective and equitable research collaborations
- Co-Design as Collaborative Research Connected Communities Foundation Series
- NIHR Guidance on co-producing a research project, March 2018
- UKRI – KFPE workshop report: Working in Effective Partnerships to Address Sustainable Development Goals
Programme management and governance
Complex programmes of global health research require significant levels of management to ensure successful delivery. It is a NIHR requirement that a full-time programme manager is appointed to manage the Centre, and sufficient resources are included and costed to manage the regular programme and financial reporting processes.
Applicants should clearly describe programme management and governance arrangements which should represent international best practice. Sufficient resources should be allocated to manage the programme/work streams from initiation to completion. This includes but is not limited to: contracting, due diligence, assurance and audit, procurement, data management, risk management (including financial, reputational and legal risks), quarterly financial reporting, monitoring, evaluation and learning, impact tracking, communication management, and compliance with ethics frameworks.
It is important to ensure the right programme management and governance support is in place for all Co-applicant institutions (LMIC, and non-LMIC), not just the Contracting Institution.
Each Global Health Research Centre will appoint its own steering committee and a diverse, independent external scientific advisory group/board. These groups should, as a minimum, have an independent Chair, be gender balanced, and have a range of members and key stakeholders with relevant expertise from the partner countries involved in the programme, as appropriate. The advisory group should advise on strategy and progress, oversee programme risks, and meet annually at a minimum. NIHR will encourage cross-representation from Centres on other Centres’ advisory groups where feasible, for mutual benefit.
NIHR expects that Centre applications will set out the respective roles and responsibilities of each Lead or Co-applicant Institution, and the researchers that represent them, following the guidance provided for equitable partnerships.
The Centre Director(s) will have overall responsibility for overseeing the scientific programme of work and all Centres are encouraged to allow early career researchers to lead on individual work packages, where appropriate. Each consortium will have nominated leads who will develop Centre-wide plans for training and capacity strengthening, CEI, MEL, and knowledge exchange, with key contacts for these in each institution. These leads will be expected to participate in the Centre’s governance.
Centres will be expected to show gender parity (ideally aiming for a 50% split) in the above positions, as well as the representation in advisory groups and governance systems.
Montitoring evaluation and Learning (MEL)
Applications should demonstrate a considered and embedded approach to monitoring, evaluation and learning (MEL), including a dedicated MEL lead, and ringfencing an appropriate level of funding to carry out MEL activities to track and evaluate progress against intended objectives.
The NIHR would encourage applicants to consider their intended pathways to impact at Stage 1 and would expect an initial draft Theory of Change for each Centre to be submitted at Stage 2. The NIHR will support successful Centres to build on these and develop them into robust frameworks for the evaluation of NCD research and research capacity strengthening activities, as part of collaborative efforts to improve learning around, and the evidence base underpinning, the delivery of the Centres.
The NIHR intends to involve Centres and MEL leads as partners in any programme-level evaluation activities and will support platforms for mutual learning as the Centres programme develops. In turn, dedicated MEL leads will be expected to consider opportunities for any relevant MEL/impact-related capacity strengthening activities to encourage and embed consideration of pathways to sustainable impact within and across Centres. For example, these could include (but are not limited to) training on developing Theories of Change, conducting stakeholder mapping and engagement, planning and undertaking local evaluations, and platforms to develop and share narrative impact case studies.
Dissemination, outputs and anticipated impact
Applicants should describe the planned outputs of the research and research capacity strengthening activities, how these will be communicated and to whom, and detail the proposed short, medium and longer term impact of the Centre. Impact is defined as the demonstrable contribution that research makes to society and the economy, of benefit to individuals, organisations and nations.
Centres are expected to have a clear and implementable strategy for pathways to impact of the proposed work, in terms of intended NCD health outcomes, and research and capacity strengthening. Examples of the types of information that could be presented in the application, and/or the kind of impacts that could be achieved, might include (but are not limited to):
- Plans for engagement with policy makers, communities and the public at an early stage.
- Individuals trained in LMIC institutions have future careers in NCD thematic areas of interest.
- Increased LMIC institutional research culture, prevalence of LMIC-led NCD research and authors in publications and new networks of LMIC experts created, resulting in significant contributions to the evidence base in the relevant NCDs.
- Research managers and support staff are also trained and retained for sustainable management and delivery of the NCD research and RCS in LMICs.
- Centre LMIC institutions win / leverage funding for NCD research through competitive processes and partnerships (e.g. with industry / philanthropy).
- Pathways to improvement in health, wellbeing, lives saved and economic, social and cultural benefits in ODA-eligible countries.
The Theory of Change provides a visual illustration of how activities, outputs and outcomes (for definitions please see explanatory notes) might be set out in a logical pathway, and thus support applicants’ own consideration of their pathways to impact. NIHR recognises that research capacity strengthening initiatives are themselves complex interventions, and encourages applicants to refer to various sources noted above for more in-depth explorations of principles and frameworks relevant to planning these kinds of activities.
Applicants will need to discuss and agree the planned or anticipated outputs, outcomes and impacts that could be realised through their Centre’s research and RCS in NCDs. It would be ideal to know what and how the Centre is expecting to contribute to advancing the health of patients and the community, as well as healthcare services in the ODA-eligible country(ies). Where possible, please quantify the potential benefits/value, the anticipated timescale for these benefits to be realised, and how the Centre’s work will create an enduring impact in the ODA-eligible country(ies).
Note: Although Global Health Research Centres will operate as single awards to consortia, all the funded Centres, their participating institutions and individual award holders, will be encouraged to consider cross-working (where common NCD themes are to be addressed), collaborating with other local/regional NCD research and research capacity strengthening initiatives, and to share best practice and training opportunities. This should help to ensure that each Centre becomes greater than the sum of its parts, and amplify the collective impact of the cohort of Global Health Research Centres.
Please refer to the NIHR Global Health Research Programme Core Guidance for information on NIHR’s expectations relating to:
- Approach to risk management and assurance
- Research contract and collaboration agreements
- Intellectual Property (IP)
- Regulatory approvals / compliance
- Reporting requirements (including equality, diversity and inclusion)
- Success criteria and barriers to proposed work
- Community Engagement and Involvement (CEI)
- Finance (including value for money)
Whilst specific information on the above sections is not required at Stage 1, it is strongly recommended that you ensure you understand the requirements for Centres at this stage and develop your application in line with the NIHR’s expectations.
Completing your NIHR Global Health Research Centres application online
Please refer to the Guidance for Completing Your Application. A Word template of the Stage 1 Application Form is available for reference only.