
Aim
NIHR has developed a Theory of Change to visually represent the Global Health Research Portfolio and the logic through which the portfolio aims to bring about its intended outcomes and impacts.
Although Theories of Change are inevitably simplifications of a complex reality, the process of developing them can help to collectively clarify the intended outcomes of an intervention, strategy or policy, identify any underlying assumptions and risks, and can be used for evaluating how our expectations played out and to understand why something works or doesn’t work in the way we initially intended or expected.
Theory of Change
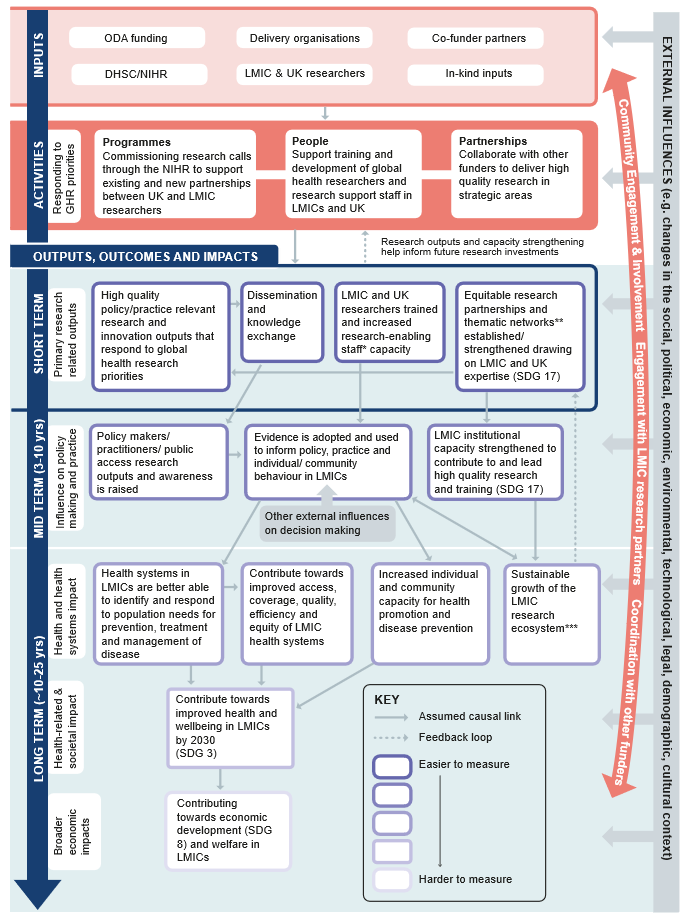
This Theory of Change is a visual representation of the logic through which the NIHR Global Health Research Portfolio aims to bring about its intended outcomes and impacts. The Theory of Change is presented in the form of a flow diagram that links inputs, activities, outputs, outcomes and impacts.
View an accessible version of the Theory of Change image
Inputs
The first stage of this Theory of Change focuses on inputs, which are:
- Official Development Assistance (ODA)
- funding, Department of Health and Social Care (DHSC)/NIHR
- Co-funder partners
- Delivery organisations
- In-kind inputs
- Researchers in low and middle income countries (LMICs) and the UK
Activities
These inputs then feed into the second stage consisting of three activity strands that respond to global health research priorities:
- Programmes - commissioning research calls through the NIHR to support existing and new partnerships between UK and LMIC researchers
- Partnerships - collaborating with other funders to deliver high quality research in strategic areas
- People - Supporting training and development of global health researchers and research support staff in LMICs and the UK
Note that the People strand overlaps with Programmes and Partnerships, because both entail capacity strengthening elements.
Outcomes
Short term
There is an arrow indicating the causal flow linking the activities to the third stage – this consists of the intended short-term outputs, which are the tangible, measurable products, goods and services resulting from the activities. For the Global Health Research Portfolio, outputs consist of two main strands:
- any high quality policy or practice relevant research and innovation outputs that respond to global health research priorities (such as publications, policy briefs, social media outputs), leading to dissemination and knowledge exchange activities
- UK andLMIC capacity strengthening activities, and establishing and/or strengthening equitable research partnerships and thematic networks (defined in line with Sustainable Development Goal [SDG] 17 – ‘Enhance North-South, South-South and triangular regional and international cooperation on and access to science, technology and innovation and enhance knowledge sharing on mutually agreed terms’).
There is a feedback loop from research and capacity strengthening outputs back to the activities in the theory, as these short-term outputs will help inform future research investments.
Mid term
In the fourth stage (mid term outcomes, approximately 3-10 years), we would expect to see short term dissemination and knowledge exchange activities contributing towards policy makers, practitioners and the public accessing these research findings and awareness being raised. This may then result in findings influencing policy, practice, and individual and community behaviour in LMICs (although other external factors will also be influencing decision making).
Long term
In the fifth stage (long term impacts, approximately 10-25 years), we would expect these changes in policy, practice and behaviour to contribute towards strengthened health systems and increased individual and community capacity for health promotion and disease prevention. Ultimately, we expect these to contribute towards improved health and wellbeing in LMICs by 2030 (in line with SDG 3) and contribute towards economic development and welfare in LMICs.
On the capacity strengthening and equitable partnerships strand, in the fourth stage (mid-term outcomes) we would expect to see evidence of strengthened capacity within LMIC institutions to contribute to and lead high quality research and training. In the fifth stage (long term impacts), we would expect this to contribute towards sustainable growth of the LMIC research ecosystem. ‘Research ecosystem’ refers to researchers and their outputs, research institutions, funders, policy makers who use the research to inform policy, communication specialists who share findings with the public, and private sector companies who develop products and employ researchers.
Growth of the LMIC research ecosystem will in turn feedback to the third stage (outputs) to help strengthen equitable partnerships and thematic networks, and may also encourage the adoption of evidence to inform policy, practice and behaviour.
Note that each of the elements above will be measured, however as we move from stage three down to stage five, these will get progressively harder to measure over time.
Cross-cutting activities
There are a number of cross-cutting activities that run across every stage of the Theory of Change. These activities will be monitored because they are expected to contribute towards the likelihood and speed of achieving the intended outcomes and impacts.
The cross-cutting activities are:
- Community engagement and involvement (CEI) through the project cycle to encourage sustainable uptake and to help in identifying any unintended (and potentially negative) impacts of the research as early as possible.
- Engagement with LMIC research partners in identifying research priorities, design/planning, implementation, analysis, and reporting and dissemination, in line with our core principle of promoting equitable partnerships.
- Coordination with other funders to drive coherence, increase impact and minimise duplication of activities.
There are also cross-cutting external influences (such as changes in the social, political, economic, environmental, technological, legal, demographic and cultural contexts), which will need to be actively monitored as they may influence whether or not the portfolio activities achieve their intended impacts.
Assumptions
The Theory of Change process has helped in identifying some of the underlying assumptions and risks around the intended causal links. These assumptions include:
- Areas of investment reflect LMIC priorities (i.e. our mechanisms for identifying global health research priorities/ engaging with LMIC policy makers and practitioners are effective)
- Global health research funders continue funding at present rate
- Funding supports LMIC leadership
- Research outputs consider access, coverage, quality, efficiency, equity.
- Activities are efficient and contribute to value for money, maximising the resources available to them.
- Researchers have skills, knowledge and networks to disseminate findings effectively to policy makers/ practitioners
- Policymakers/ practitioners have the resources and ability to understand and use research
- Individuals who participate in training are retained in domestic research system
- NIHR funded activities will have a sustainable long-lasting legacy.
If any of these assumptions do not hold true, there is a risk that this will cause a break in the causal links which may undermine the achievement of the intended outcomes and impacts. It will be important to monitor each of these assumptions and risks to test whether or not they hold true, and if any mitigation is required.
Lastly, it will be important to actively monitor any other external influences that may influence whether or not the portfolio activities achieve their intended impacts.
How this theory was developed
This Theory of Change has been developed collaboratively through a series of workshops with key stakeholders including DHSC’s Global Health Research team, NIHR Coordinating Centres, other strategic delivery partners and award holders. The Theory of Change has also been reviewed against the existing literature on pathways to health research impact.
Next steps
NIHR intends to regularly review and update this Theory of Change as evidence is gathered through the lifetime of the Global Health Research portfolio. The Theory of Chance will form the basis of ongoing and future monitoring and evaluation activities.