
NIHR Programme Grants for Applied Research (PGfAR) is seeking to increase the diversity of study type and design submitted for funding. This case study outlines a novel research design for improving the quality of maternity care through national studies of 'near-miss' maternal morbidity.
Programme details
Researcher: Professor Marian Knight
Institution: NHS Oxfordshire CCG
Funding: £1.9m, 2010 - 2016
Patient and clinical need
Many severe maternal morbidities, such as uterine rupture and maternal sepsis, have a life-long impact on the surviving women and their families, and can become the subject of litigation claims. Although individually rare, when considered together, near-miss maternal morbidities represent a considerable burden to women, their families and health-care systems.
Understanding how the NHS maternity care services can further improve the safety of women and babies is crucial.
Aims of the programme
Beyond maternal death: Improving the quality of maternity care through national studies of 'near-miss' maternal morbidity aimed to comprehensively study rare near-miss events in pregnancy (such as uterine rupture and maternal sepsis) in order to help prevent them and improve the outcomes for women and their babies through improvements to the treatments they receive and the services provided.
Programme design
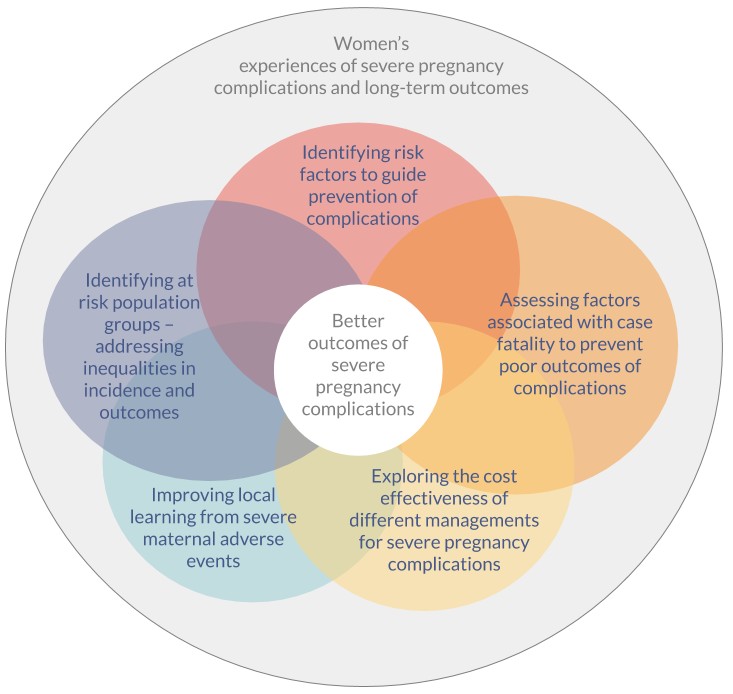
Uncommon obstetric events are by definition difficult to study, and require a national approach to generate the most robust evidence to improve care. Delivering better outcomes from severe pregnancy complications requires consideration of a range of aspects, including prevention of the condition itself, women’s experiences of care, optimal and most cost-effective treatments, and avoidance of inequalities as well as severe and long term outcomes.
The research team sought to capitalise on a national observational research platform to address all these facets to strengthen the understanding of how NHS maternity care services can further improve the safety of women and babies. A programme grant with a number of workstreams provided the ideal route to undertaking this comprehensive approach. These six workstreams are described in the text and image below.
Workstream 1
Workstream 1 used primary data collection to conduct descriptive and case-control studies to establish the incidence and identify risk factors, management and outcomes, to guide prevention of complications such as of uterine rupture, placenta accreta, HELLP syndrome, septicaemic shock and amniotic fluid embolism.
Workstream 2
Workstream 2 used logistic regression analysis of previously collected maternal deaths data and near-miss morbidity data to assess factors associated with case fatality, to prevent poor outcomes of complications.
Workstream 3
Workstream 3 identified at risk population groups, to address inequalities in incidence and outcomes of near-miss maternal morbidity.
Workstream 4
Workstream 4 explored methods for improving local learning from severe maternal adverse events.
Workstream 5
Workstream 5 undertook a pilot economic evaluation to explore the cost-effectiveness of different management approaches for severe pregnancy complications such as peripartum haemorrhage.
Workstream 6
Workstream 6 explored women’s experiences of severe pregnancy complications and long-term outcomes.
Summary of findings
The contribution of existing risk factors to disease incidence, and steps that may be taken in clinical practice to address these factors to reduce incidence, were investigated. Signs of severe sepsis, particularly with confirmed or suspected group A streptococcal infection, should be regarded as an obstetric emergency and should be routinely included in obstetric emergency training courses. A number of recommendations were made for management of specific conditions; for example, women who have placenta praevia and have had a previous caesarean delivery are at very high risk of placenta accreta and delivery should be managed by specialist teams accordance with this risk.
The impact of different management strategies or interventions on outcomes and costs was analysed, and recommendations for best practice to improve outcomes. Amongst the many findings, uterine compression sutures were found to be a more cost effective second-line therapy for post-partum haemorrhage than interventional radiology, and guidelines should reflect this.
What has happened as a result?
A number of national and international guidelines, including the NICE caesarean section guideline CG132 and the WHO recommendations for prevention and treatment of maternal peripartum infections, were influenced by the research findings.
Key statistics and publications derived in this award were cited in Annual Report of Chief Medical Officer, 2014 ‘The Health of the 51%: Women’. Marian Knight was a co-author of Chapter 8 ‘Post pregnancy care: missed opportunities during the reproductive years’.
Find out more
- Final report
- Healthtalkonline module - Conditions that threaten women’s lives in childbirth & pregnancy
- EuropePMC - linked 30 publications to this award