
NIHR Programme Grants for Applied Research (PGfAR) is seeking to increase the diversity of study type and design submitted for funding. This case study outlines a novel research design for angina and heart attack.
Programme details
Researcher name: Professor Harry Hemingway
Institution: University College London Hospitals NHS Foundation Trust
Funding: £2m, 2009 - 2015
Patient and clinical need
Coronary heart disease (CHD) is the main cause of preventable, premature mortality in the world. However, patients suffer because there are variations in prevention, investigation and treatment between hospitals, professionals and socio-demographic groups. There are a lack of large-scale outcome studies using samples of nationwide data meaning surprisingly little is known about how patient outcomes are affected during the patient journey.
CHD is one disease area in which large-scale, detailed and diverse data (‘big data’) exist and may provide new opportunities for understanding quality of care and outcomes.
Aims of the programme
Improving the quality of care of patients with angina and heart attack aimed to link and use electronic health records (EHRs) from primary care, hospitalisations and national registries in cardiovascular disease to identify opportunities to improve outcomes for patients with stable coronary artery disease and acute coronary syndrome.
By building an EHR research resource, the team hoped to identify the most important opportunities to improve patient care and find out how variations affect patient outcomes. In addition, the team aimed to identify cost-effective improvements in chest pain clinics and determine the cost effectiveness of new blood tests for novel biomarkers.
Programme design
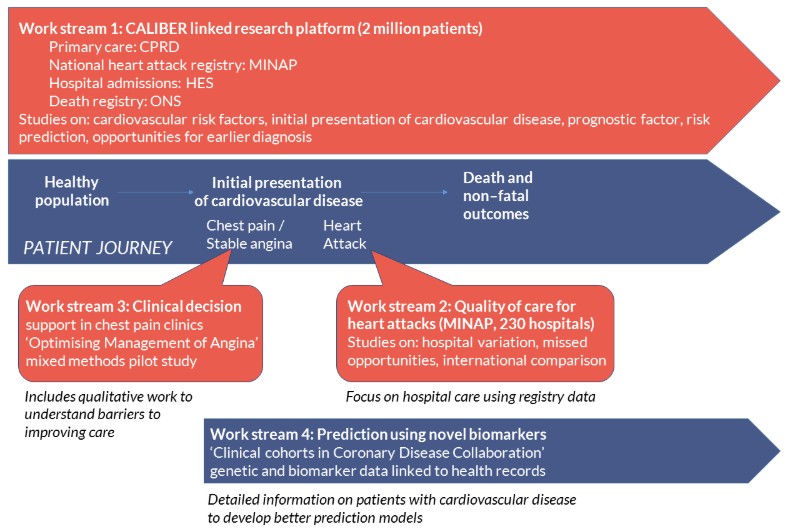
The programme followed the patient journey for angina and heart attack, with a linked electronic health record research platform (CALIBER: Clinical disease research using linked bespoke studies and electronic health records) at its core. CALIBER contains information on the health population in primary care, and follows patients through to hospitalisation, death and other outcomes. The programme comprised 33 inter-related studies, combining methods from epidemiology, health informatics, health economics and ethnographic social science approaches.
Workstream 1
Workstream 1 developed the CALIBER platform and used it to better understand risk factors, initial presentation of cardiovascular diseases and prognostic factors. CALIBER was used to develop risk prediction tools, identify opportunities for earlier diagnosis and preventative care, and quantify treatment benefits as an alternative to randomised controlled trials.
Workstream 2
Workstream 2 focused on hospital care for myocardial infarction (heart attacks), with studies on hospital variation, missed opportunities for care and international comparisons. It used the full Myocardial Ischaemia National Audit Project (MINAP) database, looking at all heart attack hospitalisations in England.
Workstream 3
Workstream 3 developed and piloted the Optimising Management of Angina (OMA) intervention, a computerised clinical decision support system for use in rapid access chest pain clinics, and also included ethnographic analysis to understand the barriers to improving care.
Workstream 4
Workstream 4 established a cohort of patients with suspected stable coronary artery disease with linked genetic, biomarker and health data, and evaluated biomarkers as prognostic indicators in stable coronary artery disease.
Why was this programme design chosen?
Individual sources of health data have weaknesses, and no single source can fully illustrate the patient journey, but linkage of multiple data sources (as in the CALIBER programme) can overcome these weaknesses. EHR databases need to be converted to a research-ready format and validated before they can be used, which was a significant component of workstream 1.
Workstreams 2 to 4 were designed to study elements of care that were not captured by CALIBER: the workings of frontline services in a chest pain clinic, studying hospital outcomes in detail (across all acute hospital in England) and investigating biomarkers that are not currently measured routinely in clinical care.
Summary of findings
A novel research platform called CALIBER was created, involving linkage of four EHR data sources and over 600 phenotyping algorithms for diseases and risk factors. It allows the wealth of information stored in EHRs to be utilised for research.
Studies performed using CALIBER identified opportunities to improve diagnosis andrisk stratification, and offer cost-effective treatment for people with CHD. A pilot study in chest pain clinics highlighted the challenges in implementing decision support systems, and biomarker studies demonstrated potentially useful prognostic indicators.
Although this study focused on cardiovascular diseases, the approach could be widely applicable to many other diseases. However, the main barrier remains the inaccessibility of the majority of NHS data, particularly in secondary care.
What has happened as a result?
CALIBER has been further developed and has become a leading research platform for the understanding of health progression, and has so far supported over 70 research projects spanning rare and common conditions. The resource now comprises more than 10 million adults with 400 million person-years of follow-up, disease and risk factor phenotyping algorithms, methods, tools and scripts, specialised infrastructure and training and support. CALIBER enables researchers to recreate the patient journey (‘from cradle to grave’) through care pathways to study disease onset and progression.
The investigators from this award successfully established the Farr Institute London (led by MRC), which has subsequently informed national and international public health policy and become part of Health Data Research UK. The work influenced NICE guidelines on chest pain of recent onset and on management of stable angina, changing the diagnostic pathway of patients with suspected stable angina and leading to recommendations about the need to assess psychosocial factors including depression in people with myocardial infarction. These are the strongest recommendations to date that clinicians might consider psychosocial factors in addition to the better recognised behavioural and biological factors.
Find out more
- Final report
- Project website
- EuropePMC - linked 62 publications to this award