
Timetable and Budget
| Description | Deadline/Limit |
|---|---|
| Deadline for Stage 1 Applications | 04 October 2022, 1 PM |
| Notification of outcome of Stage 1 Application | 13 December 2022 |
| Deadline for Stage 2 application | 24 January 2023, 1 PM |
| Notification of outcome of Stage 2 Application | June 2023 |
| Project Start | July 2023 |
| Project Duration | 24-30 months |
| Budget | £1.7m-£2m |
Introduction
In December 2021, the government announced a new 10-year drug strategy ‘From Harm to Hope’. The strategy is built around three strategic priorities (1) to break drug supply chains, (2) to deliver a world class treatment and recovery system, (3) to achieve a generational shift in demand for drugs, and sets out a whole-system approach to tackling illegal drug use, and reducing drug-related harm, death and crime in England. Three separate portfolios of work have been developed to deliver against these priorities. The Department of Health and Social Care (DHSC) is leading work to deliver world-class treatment and recovery services for substance users within the next decade, supported by the Ministry of Justice (MoJ), the Department for Levelling up, Communities and Housing (DLUCH), and the Department for Work and Pensions (DWP).
The ambition to build a world class treatment system will be delivered through the Treatment and Recovery (T&R) Portfolio, which is underpinned by £780 million of new funding over a three-year period. The majority of this investment (£532m) has been allocated to DHSC to distribute to Local Authorities, to fund the transformation of community treatment and recovery services, with smaller allocations being made available to deliver additional elements of the recovery package. This funding includes £120m for MoJ to improve offender treatment pathways, £30m for DWP to strengthen the employment offer for those receiving drug treatment, and £68m allocated to DLUCH to implement new housing support services.
The T&R portfolio includes six key strands of work. Within each work strand sit a number of programmes designed to deliver different elements of the improvement package. For more information on the structure of the portfolio please see Annex A.
DHSC led work strands within the portfolio (see annex A) are focused on expanding local authority commissioned substance misuse treatment services including satellite support services (e.g., housing and employment support), and embedding recovery support and communities into every local area. Local authorities can use the new funding to invest across a range of services and interventions to improve service quality, expand treatment capacity, rebuild the workforce, and strengthen specialist services for children and young people.
As part of the drug strategy funding settlement from HM Treasury, departments with responsibility for delivering the portfolios are required to carry out evaluation as part of their work plans. DHSC is committed to conducting high-quality evaluation of its policies, programmes and projects, and through The National Institute for Health and Care Research (NIHR) Policy Research Programme (PRP), invites applications for a single research project to design and deliver the evaluation of the Treatment and Recovery Portfolio.
This research will be critical for evaluating a significant national multi-year portfolio of work, and would be required to assess the portfolio’s overall implementation, and carry out several smaller scale appraisals for a select number of high priority programmes. The portfolio will need to be evaluated for the duration of the new investment (2022/23 to 2024/25), and we therefore expect the project to run until summer 2025, with a substantive interim report estimated to be due in summer 2024 (ahead of the next Spending Review - exact timings are TBC), and a final report due in Autumn/Winter 2025. In the context of the 10-year strategy, this is an opportunity to provide robust evidence to inform future policy and portfolio development, and support the next phase of delivery planning to ensure that people living with drug dependence are given the best chance to achieve and maintain recovery.
There are two MoJ led work strands within the portfolio which focus on improving drug treatment and recovery provision in Prisons, and within the Community Justice and Probation system. We are expecting that these aspects will be evaluated separately by MoJ. Whilst applicants should concentrate their proposal on designing a robust evaluation of the DHSC-led work strands which relate to the community treatment and recovery system, we would also want proposals to include a consideration of DHSC activities to strengthen offender pathways into community services. We would encourage the successful applicant to join up with MoJ’s evaluation team where feasible and relevant to ensure evidence on the intersection between criminal justice and community treatment systems is sufficiently captured.
Background
In England, there has been a rising trend in drug misuse and drug-related deaths over recent years. Drug misuse deaths are now the highest on record (2,846 deaths registered in 2021) and are 91% higher than in 2012 (1,492) [1]. The impacts of drug misuse extend beyond the direct harms to the individual drug user, with the combined cost of illicit drug use to society estimated to be over £19 billion [2]. Disinvestment in the drug treatment system since 2013/14 has resulted in a decline in the capacity and quality of treatment available, which has contributed to worsening outcomes for drug users, and increasing levels of unmet need.
The harms caused by drug misuse are not distributed evenly across the country, and are strongly linked to deprivation. Many of the highest prevalence rates for opiate and/or crack cocaine use are in the north of England, and 56% of those in treatment for crack and/or opiates are living in places ranked in the 30% most deprived areas in England [3]. Rates of drug misuse death have a marked regional divide, with the North East having consistently the highest drug misuse mortality rate for the past nine years. In 2021, the drug misuse death rate in the North East (104.1 deaths per million) was three times higher than the rate in London (32.5 deaths per million), and nearly four times higher than the death rate in the East of England ( 27.4 deaths per million) [4].
In February 2020, part one of Dame Carol Black’s independent review of drugs was published, providing an in-depth analysis of the scale of the drug issue in England, and of the challenges posed by drug supply and demand. In July 2021, part two was published, which focused on treatment, recovery, and prevention, and made wide ranging recommendations to government on improvements to the substance misuse treatment and recovery system.
Government accepted these recommendations and published the new drug strategy in response to the independent review, as well as guidance for local delivery partners on how this new approach should be applied at the local level. Within the strategy, government has also set out a group of core outcomes and targets which portfolios are expected to deliver against.
The Treatment and Recovery portfolio activities are expected to play a pivotal role in achieving the outcomes listed below:
- Reduced drug related harm (health and social)
- Reduced drug use
- Increased engagement in treatment
- Improved recovery outcomes
- Reduced drug-related crime (through getting more individuals in treatment)
A separate piece of work will be carried out alongside the evaluation to monitor progress against the National Combating Drugs Outcomes Framework and supporting metrics which will be published later this year.
The majority of the portfolio’s funding will be delivered through supplemental funding using section 31 grant mechanisms. Via these mechanisms, a universal fund will be distributed to all local authority areas to provide an uplift in drug treatment funding, and an additional supplementary fund will be distributed to local authorities in waves through a phased roll out across the three year funding cycle. This phased approach will target local authorities with the poorest drug-related outcomes and highest levels of deprivation first, with 50 local authorities receiving the additional funding in the first year, 50 more in the second, and the remaining 50 in year three. This approach has been developed to reduce the large geographical inequalities in drug misuse outcomes that exist, by targeting areas with the greatest level of need. The additional drug and alcohol treatment funding allocations for 2022 to 2023 have been published and set out the 50 areas included within the first enhanced funding tranche.
Local authorities are required to make decisions on how the new funding is used within their area based on the needs of the local population. DHSC’s Office for Health Improvement and Disparities (OHID) has provided local authorities with a menu of interventions which sets out the services and interventions which are eligible for funding to enable local authorities to develop their service delivery models and spending plans. Local authorities are then required to submit their spending and delivery plans to OHID.
Research priorities
This research is expected to have two strands of work:
- Research strand 1: An overarching process evaluation of the treatment and recovery portfolio which takes a whole-system perspective to assessing the implementation of portfolio activities.
- Research strand 2: Evaluation of a smaller number of programmes in areas identified as high priority to appraise the delivery of individual programmes and develop the evidence base.
Research strand 1: Overarching evaluation
The overarching evaluation should focus on evaluating the implementation and delivery of the portfolio. An overarching assessment of the portfolio’s impact and value for money will be carried out separately by DHSC, and we therefore do not expect these elements to be included as part of this piece of research (for more information on DHSC’s plans for conducting an impact and economic evaluation, please see annex b). We would however expect the successful applicant to work collaboratively with DHSC’s evaluation team to optimise evidence collection and learning opportunities across the evaluation piece. We anticipate findings from this research will be critical for supporting the impact evaluation by building a rich picture of the factors influencing outcomes and how these vary across contexts and geographies, and by helping to explain how and why observed changes in outcomes have occurred.
This research should include a process evaluation which assesses the implementation of the portfolio to understand if programmes have been implemented and delivered as intended, how implementation varies across contexts, and to explore how the programmes impacted the intended outcomes (and contributed to any unintended outcomes and/or consequences). The evidence gathered through the process evaluation will be critical for (1) assessing if any changes need to be made to the portfolio to produce the intended outcomes, both in the short and long term, (2) to inform future policy and service delivery decisions, and (3) to help explain findings from DHSC’s impact evaluation.
The process evaluation should therefore look to consider questions around:
- Identifying the challenges, barriers, and enablers of implementation and delivery on the ground
- Understanding how contextual factors, such as Covid, influenced delivery
- Understanding what processes did and didn’t work, for who, where, and why
- Identifying areas and/or mechanisms for improvement
- Identifying effective pathways of change through applying findings to evidence of portfolio impact to understand how outcomes have been achieved
Applicants should ensure that OHID activities to strengthen offender pathways into community treatment services (see Annex A) are included within the scope of the overarching evaluation. As part of the menu of interventions (see paragraph 15), local authorities have been given the option of investing in different interventions to increase the integration of, and improve care pathways between, criminal justice settings and drug treatment services. We are therefore interested in evaluating the implementation and delivery of these OHID activities to understand if, how, where, and why these have contributed to improvements in drug treatment and recovery outcomes for individuals within the criminal justice system.
Applicants should also note that DWP are carrying out an evaluation of the Individual Placement Support programme (an employment support intervention), which sits within the wider High Class Community Treatment and Recovery System work strand of the portfolio. We therefore do not expect this research to include an in-depth appraisal of the employment support programmes, however we would want these interventions to be included as part of this overarching process evaluation, as they are considered to be an important component of the extended treatment and recovery package, and new whole system approach.
Although open to other methodologies, we anticipate that the process evaluation would use qualitative research methods to explore portfolio implementation within a sample of local authority areas. In choosing the sample, applicants should ensure it provides adequate representation across geographies, models of service provision, and funding tranches. OHID have strong links with local authorities and can provide relevant contextual information to support the development of an appropriate sample, we would therefore encourage the successful applicant to engage closely with OHID ahead of final selection.
Research strand 2: Evaluation of selected programmes
Several programmes within the portfolio have been identified as areas of high priority for this research project. These programmes, which are outlined in more detail below, are areas where significant evidence gaps exist and/or have been newly developed as a result of the drug strategy funding package. A programme-specific evaluation is therefore required in each of these areas to examine whether they have been implemented and are working as intended, and to understand the contribution they are making to observed changes in patient outcomes.
Programme specific evaluations:
Housing support: As part of the T&R investment package, funding has been allocated to improve the housing support offer for those using substance misuse treatment services. The investment will fund a new suite of interventions to improve access to, or sustain, suitable and safe accommodation. As this is a newly developed policy, not all local authorities will be eligible for the additional housing support investment during this funding cycle. The 28 local authorities who will receive this investment have been selected based on their level of housing need and their geographical distribution to ensure there is sufficient regional coverage. This research will therefore be important for building the evidence base on this new housing support offer. The research requirements for the housing support programme include:
- An assessment of the implementation and delivery of new housing support services which should explore issues such as if implementation was carried out as intended, what barriers and facilitators were experienced on the ground, what did and did not work (for who, where, and why), and how the wider and local context influenced delivery.
- An assessment of the impact of the housing support programme which explores how housing support services have contributed to changes in health outcomes in service users, including the identification of any unexpected outcomes.
Workforce: The drug and alcohol treatment and recovery workforce transformation programme aims to improve the capacity, composition and quality of the drug and alcohol treatment and recovery workforce through a range of new initiatives. The research requirements for the workforce programme include:
- An assessment of contextual and attitudinal factors which influence employees’ perceptions and experiences of working within the drug and alcohol treatment and recovery system. As examples, this could include: Influential factors in decisions to join or leave the drug and alcohol treatment workforce; Staff morale; Staff satisfaction including issues around progression, supervision, pay, pension, and benefits packages; and staff education, training and skills.
- To examine if and how these contextual and attitudinal factors are changing over the course of the delivery of the workforce transformation programme.
Recovery communities: The recovery communities programme involves the development and expansion of recovery communities and peer support networks to facilitate sustained long-term recovery, increased visibility of recovery, and to support social integration for those who have previously been or are currently living with drug dependence. The research requirements for the recovery communities programme include:
- To explore what recovery support services (RSSs) contribute to systems of care and how effective they are in sustaining recovery outcomes.
- An assessment of the impact and contribution of Lived Experience Recovery Organisations (LEROs) on recovery outcomes, including treatment reintervention where required.
- An assessment of whether LEROs offer value for money.
Service integration: A programme of work in partnership with NHSE/I is being undertaken to address co-occurring drug and alcohol use, mental health, and physical health. A number of areas of work are being explored, including the Joint Action Plan between OHID and NHSE/I, as recommended by Dame Carol Black. This work is evolving, and exact deliverables are still being agreed. Programme aims include (1) improving mental and physical health treatment provision and quality for drug and alcohol users, (2) improving the earlier detection of co-occurring conditions and treatment pathways available for individuals with a drug dependence. Once activities within this space have been finalised, OHID will share more information with applicants to inform their thinking on this programme’s appraisal, however broadly we anticipate the research requirements for the service integration programme to include:
- To explore how programme activities have impacted service delivery and joined up working across physical, mental, and substance misuse treatment services, and to identify what can be improved in future years.
- To identify new models of working, or change in practice, for co-occurring mental and physical health conditions and to examine the extent to which services are better integrated and treatment pathways more established.
Buvidal provision: Local authorities have been given the option to invest in piloting and/or increasing provision of novel long-acting opioid substitution treatments (e.g. Buvidal) within their treatment services. Evidence of the effectiveness of Buvidal treatment primarily comes from a Randomised Control Trial by Lowfall et al. (2018). NICE have also carried out an evidence review, and have concluded that Buvidal is a viable treatment option in the treatment of opioid dependency. Whilst Buvidal is not currently widely used within drug treatment services in England, it is anticipated that all local authorities will choose to introduce and/or increase provision of Buvidal over the next three years as part of their spending plans, with the majority expected to do so from the first year of funding. Given this, we would be looking for this research to build the evidence base on the use of Buvidal treatment in practice (please note applicants would not be expected to carry out an RCT). The research requirements for Buvidal provision include:
- To identify the challenges, barriers and facilitators to implementing and delivering Buvidal treatment, and achieving treatment uptake in the target population.
- To explore patients’ experiences of and attitudes to receiving Buvidal treatment.
- To identify the characteristics of patients who benefit most from Buvidal treatment, and the characteristics of those who don’t.
- An assessment of what differential impact the new or increased provision of Buvidal has had on patient outcomes.
- To explore what, if any, unintended consequences have arisen as a result of introducing and/or increasing Buvidal provision.
- To determine the relative costs of providing Buvidal compared to other opiate substitution therapy treatment options.
Increased Buvidal provision is also expected to be made available within criminal justice treatment services. If feasible, we would want this research to consider Buvidal treatment as part of the appraisal of offender service integration, and pathways of care for those leaving treatment services within secure settings and entering the community treatment system. We are interested in exploring questions around the effective management of, and any issues around, the continuation of Buvidal treatment for patients when moving from one setting to another.
New Guidance on Health Inequalities data collection within NIHR PRP Research:
Health Inequalities is a high priority area within the Department of Health and Social Care and the NIHR and is often present in a majority of funded projects. We are now assessing all NIHR research proposals in relation to health inequalities. We are asking applicants to identify in their application whether or not there is a health inequalities component or theme and how this research hopes to impact health inequalities. We are also asking researchers to collect relevant data, if appropriate for the research. Our goal is to collect information on health inequalities in research and data relating to the main outcome(s) of the proposed research. Please clearly identify in this section whether or not your application has a health inequalities component or relevance to health inequalities and detail the core set of health inequalities breakdowns that will be reported; if none please explain why. We understand that research projects have different methodologies and focus on different populations, so please explain what data will be collected and reported for the methodology you plan to use. If a health inequalities component is not included, please explain why this does not fit within your proposed research. This should only be a few sentences.
For quantitative research we would ideally like researchers to provide one-way breakdowns of their main outcome(s) by the following equity-relevant variables: age, sex, gender, disability, region, 5 ONS Ethnic groups, and the 5 IMD quintile groups. If more detailed cross tabulations are appropriate, please include these. This table should be submitted to NIHR PRP at the end of the project. Due to data limitations, judgement calls may be necessary about which breakdowns to report and whether to merge categories to increase counts in particular cells; we ask you to make these judgement calls yourself, bearing in mind our data curation aim of enabling future evidence synthesis work in pooling results from different studies. More details and an example table can be found in Appendix A.
For qualitative research projects, this can be purely descriptive statistics giving the number of observations against the various variables.
Further details about this new request can be found in Appendix A.
We will also be holding a Health Inequalities in NIHR PRP Research Q&A Event on 19 September 2022, more details in APPENDIX B.
Challenges
We recognise that this research request has some significant challenges, particularly associated with being able to robustly evaluate the impact of the portfolio and the individual programmes within it, and we are open to suggestions on how to best navigate these challenges to produce valid and informative evidence to support future policy, service delivery, and spending decisions.
The key challenges identified are set out below:
- The mechanisms by which the programmes and interventions within the portfolio will be delivered have already been agreed, and there is limited opportunity to influence this going forward due to implementation processes already being underway.
- Local authorities are required to select which services and interventions they want to invest in based on a menu of interventions which sets out the different services and interventions which are eligible for funding. This menu has been developed by OHID, and is evidence based with the treatment interventions backed by NICE and clinical guidelines. However, the ability for local authorities to choose both which services, and the extent to which these services will be invested in based on their population needs and what they do or do not already have in place, raises a significant challenge in developing a comparator group, and being able to attribute impact, given the variety of different service delivery models which are expected to emerge. DHSC will therefore be taking a high-level approach to assessing impact, and will not be looking to attribute changes in patient outcomes to individual programmes or interventions.
- Local authorities will start receiving money from the new investment in July 2022. We recognise this poses a significant challenge to capture any baseline data for the programme-specific evaluations or new measures of interest as service implementation and delivery will be able to begin on receipt of the funds.
- We recognise that this is an ambitious research request that is both broad in scope and complex in its requirements, however due to the multiple links and interdependencies between programmes within the portfolio, we are commissioning this research as a single project. We are open to suggestions on the most suitable approach to generate insights across these different requirements, and encourage applicants to clearly outline in their proposals how they will address all the different elements set out within the research priorities section of this specification.
- The funding allocation has been confirmed for the next three years, however we anticipate significant additional funding will be required to be able to meet the commitments set out within the 10-year drug strategy, and to ensure that any gains achieved through this investment are not lost. Having evidence to support the next Spending Review (estimated autumn 2024) is therefore a key driver for this work, and we would require an interim evaluation report outlining preliminary findings to be available prior to spending review launch (estimated to be due in summer 2024). Producing sufficient evidence on impact and VfM under these compressed timelines will be extremely challenging, and we are therefore expecting to rely on evidence from the process evaluation element of this research, as well as information gathered through the separate monitoring exercise, to inform SR processes.
Areas out of scope for this programme of work
As outlined in the introduction section, we are expecting the MoJ led work strands to be evaluated as a separate project. For the purpose of this research, programmes within the T&R portfolio relating to Prisons and Community Justice and Probation (see annex A) are considered to be out of scope, except those activities being led by OHID which are directly linked into community treatment services. We would encourage the successful applicant to engage with MoJ’s evaluation team given the cross overs and interdependencies between the Criminal Justice, and community treatment systems.
As outlined in the research priorities section, an overarching impact and economic evaluation will be carried out by DHSC (see annex B for more information), an assessment of the impact and value for money of the portfolio which takes a whole system approach is therefore out of scope for this research. Applicants should however consider impact and economic appraisal of the selected individual programmes where this has been specified in the research priorities section above, and ensure that this is addressed within their proposals.
The portfolio is only being implemented in England, therefore treatment and recovery systems within the devolved administrations are out of scope. We are however open to using devolved administrations data as a comparator where feasible and appropriate.
The portfolio sits within a wider programme of work to deliver the three strategic priorities of the drug strategy. Whilst initiatives to reduce demand and supply are out of scope, we would expect the successful applicant to develop an understanding of the synergies between these programmes and the T&R portfolio in achieving intended outcomes. The T&R portfolio evaluation will also be an important element of the overall drug strategy evaluation which is being delivered by the Joint Combating Drugs Unit (JCDU), and we expect outputs from this evaluation will feed into this wider evaluation programme.
Technical requirements / Expertise required
Applicants should have, and be able to demonstrate, the following expertise:
- Knowledge of the drug treatment and recovery system in England and the policy context.
- Expertise in undertaking complex evaluations of national programmes.
- Experience in designing and conducting large scale mixed methods research projects.
- Experience working with local authorities.
- Knowledge of the National Drug Treatment Monitoring System and other drug-related data sets.
Outputs
Substantive interim report due in summer 2024 setting out initial findings and learning from the process evaluation. The interim outputs will be critical for informing the next spending review, and we would expect applicants to set out a clear plan of how they would ensure this requirement was addressed within their applications. Applicants should please also note that exact timelines for the next Spending Review are currently unavailable, therefore deadlines included within this specification should be treated as indicative and may be subject to change.
Final report due in Autumn/Winter 2025. The final report should be of a publishable standard and fully accessible to policy makers, healthcare professionals and members of the public. It will be circulated widely in DHSC, the JCDU, other government departments and arms-lengths bodies, and stakeholders involved and/or with an interest in the project.
Regular tailored briefings and reporting to explain key findings to policy officials and key/relevant stakeholders. We would expect the research team to share emerging findings throughout the project’s lifecycle, and engage regularly with DHSC’s evaluation team. Coordinating approaches across the overarching process and impact evaluation elements will be essential for developing a cohesive and comprehensive evaluation narrative which can inform policy development and/or portfolio improvement.
Applicants are asked to consider the timing and nature of deliverables in their proposals. Policymakers will need research evidence to meet key policy decisions and timescales, so resource needs to be flexible to meet these needs. A meeting to discuss policy needs with DHSC officials will be convened as a matter of priority following contracting.
Budget and duration
Applications will be assessed on value for money, we would expect them to cost between £1.7m-£2m.
The project is expected to start in Summer 2023. The evaluation research will need to cover the duration of the investment (2022/23 to 2024/25), with an interim report due in Summer 2024 and a final report due in Autumn/Winter 2025 (as noted in paragraph 38 above, output deadlines provided within this specification are provisional and may be subject to change).
Costings can include up to 100% full economic costing (FEC) but should exclude output VAT. Applicants are advised that value for money is one of the key criteria that peer reviewers and commissioning panel members will assess applications against.
Management arrangements
A research advisory group including, but not limited to, representatives of DHSC, other stakeholders (including representatives from other government departments such as DLUCH, MoJ, DWP), and the successful applicants for the research should be established. The advisory group will provide guidance, meeting regularly over the lifetime of the research. The successful applicants should be prepared to review research objectives with the advisory group, and to share emerging findings on an ongoing basis. The successful applicant will be expected to:
- Provide regular feedback on progress
- Produce timely reports to the advisory group
- Produce an interim and final report for sign off
The successful applicant will be expected to work with nominated officials in DHSC, its partners and the NIHR. Key documents including, for example, research protocols, research instruments, reports and publications must be provided to DHSC in draft form allowing sufficient time for review.
Specification Webinar
The Evaluation of the 10-year drug strategy is a high priority for the Department of Health and Social Care and the Office for Health Improvement and Disparities. Given the scale and complexity of this call, to ensure applications are high quality and meet the specification, we will be hosting a webinar for potential applicants on Wednesday 14 September, 2-3:30pm, ahead of the Stage 1 submission date. This will be hosted by CCF with DHSC and OHID colleagues via Zoom and will allow applicants to ask questions on the specification and hear more about the evaluation requirements. You can register for the webinar using the google registration form
References and key documents
- Office for National Statistics (2022). Deaths related to drug poisoning in England and Wales: 2021 registrations. [Accessed 15 August 2022]
- Department of Health and Social Care (2020). Review of drugs: phase one report. [Accessed on 15 August 2022]
- Office for Health Improvement and Disparities (2021). Adult substance misuse treatment statistics: 2020 to 2021. [Accessed 15 August 2022]
- Office for National Statistics (2022). Deaths related to drug poisoning in England and Wales: 2021 registrations. [Accessed 15 August 2022]
Annex A
Drug Treatment and Recovery Portfolio - Department of Health and Social Care (DHSC), Department for Levelling Up, Housing and Communities (DLUHC), Department for Work and Pensions (DWP) and Ministry of Justice (MoJ)
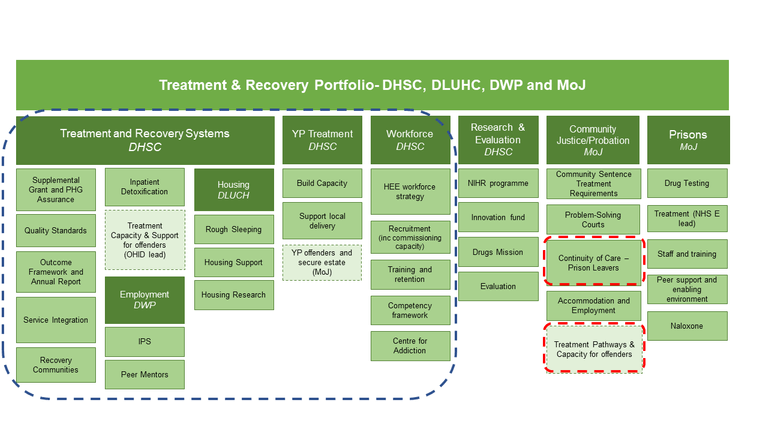
A. Treatment and Recovery Systems - DHSC. These programmes are in scope of this research
- Supplemental Grant and PHG assurance
- Quality Standards
- Outcome Framework and Annual Report
- Service Integration
- Recovery Communities
- Inpatient Detoxification
- Treatment Capacity and Support for offenders (OHID lead)
Employment - DWP These programmes are in scope of this research
- IPS
- Peer Mentors
Housing - DLUCH These programmes are in scope of this research
- Rough Sleeping
- Housing Support
- Housing Research
B. YP Treatment - DHSC These programmes are in scope of this research
- Build Capacity
- Support local delivery
- YP offenders and secure estate (MoJ)
C. Workforce - DHSC These programmes are in scope of this research
- HEE workforce strategy
- Recruitment (including commissioning capacity)
- Training and retention
- Competency framework
- Centre for addiction
D. Research & Evaluation - DHSC
- NIHR programme
- Innovation fund (Joint JCDU/OHID lead)
- Drugs Mission (Joint OLS/OHID lead)
- Evaluation
E. Community Justice/Probation - MoJ
- Community sentence treatment requirements
- Problem-solving courts
- Continuity of Care - Prison Leavers - this programme has links into the community treatment system and should be considered as part of the process evaluation
- Accommodation and Employment
- Treatment Pathways and Capacity for offenders - this programme has links into the community treatment system and should be considered as part of the process evaluation
F. Prisons - MoJ
- Drug Testing
- Treatment (NHSE Lead)
- Staff and Training
- Peer support and enabling environment
- Naloxone
Annex B
Summary of DHSC’s plan for assessing T&R portfolio impact and value for money
Impact evaluation:
DHSC’s impact evaluation will take a high-level approach to assessing impact. The new strategy aims to move away from siloed approaches to treating drug addiction by providing coordinated provision of services at the local level. We will be looking to better understand what the impact of taking a whole system approach is, and how the additionality of providing multiple interventions concurrently which are targeted to help different aspects and consequences of addiction (e.g. unstable housing, unemployment, co-occurring mental health problems), contributes to treatment and recovery outcomes. The overarching impact evaluation will consider questions around:
- Assessing the overall net impact of the portfolio in achieving outcomes
- The effectiveness of taking a whole system approach
- The impact of enhanced funding compared to universal funding
- The impact of the phased funding approach on geographical health disparities
- The impact of three-year indicative allocations on the planning process
We anticipate using a quasi-experimental design to explore the impact of the T&R portfolio funding by comparing observed outcomes with what would have been expected to happen in the absence of the new investment. We recognise the challenges associated with conducting a robust assessment of the portfolio’s impact (outlined in the challenges section of this specification), and will be carefully considering what methods would be most appropriate to produce valid and informative evidence to support future decision making in the community treatment and recovery system space.
The drug strategy sets out a transformation programme spanning a 10-year time horizon, and we are interested in evaluating the portfolio over an extended period to capture evidence on the longer-term impacts of the investment. Our priority is to gather evidence of impact on more immediate outcomes, however we will be aiming to develop replicable methodologies which would allow for extended and comparable data collection at a future time point.
We anticipate that the findings from the overarching process evaluation (set out within this research specification) will be a key source of evidence to supplement findings from the impact evaluation. The findings are expected to help develop our understanding of how, where, in what contexts, and why portfolio activities have (or have not) succeeded in improving outcomes. Critically, we would expect the process evaluation to identify the mechanisms and/or pathways by which changes to outcomes have occurred, with a focus on understanding if and how these differ across, and/or are influenced by, different contexts, geographies, and models of service provision.
Economic evaluation
An economic assessment of the costs and benefits of portfolio activities will be undertaken by DHSC to understand whether and the extent to which value for money was achieved. Through the economic evaluation we are looking for evidence on the costs and benefits realised by the portfolio as a whole, but do not expect it to include any value for money assessments of individual programmes or interventions.
Appendix A: Further Detail on the New Guidance on Health Inequalities data collection within NIHR PRP Research
Health Inequalities is a high priority area within the Department of Health and Social Care and the NIHR and is often present in a majority of funded projects. We are now assessing all NIHR research proposals in relation to health inequalities. We are asking applicants to identify in their application whether or not there is a health inequalities component or theme and how this research hopes to impact health inequalities. We are also asking researchers to collect relevant data related to health inequalities, if appropriate for the research. Collecting specific information about health inequalities in research submitted to the programme will allow for categorisation of health inequalities research, curation of data to aid future health inequalities research and enable policymakers to better understand the implications of health inequalities within their policy areas. This is a new request from the NIHR PRP and we will be continuing to monitor queries and adapt the process as needed. If you have any feedback on this new request, please contact us at prp@nihr.ac.uk.
Our goal is to facilitate more widespread and consistent reporting of health inequality breakdown data relating to the primary outcomes of NIHR funded research. We would ideally like researchers to focus on the following equity-relevant variables: age, sex, gender, disability, region*, 5 ONS Ethnic groups**, and the 5 IMD quintile groups. These variables are considered an ideal, but we understand that these are subject to change depending on the sample population and specific research question.
For qualitative research projects, this can be purely baseline characteristics of the participants, for example, the number of participants in each ethnic group.
For quantitative research projects, if there are multiple outcomes/effects with your stakeholders, select a small number of main outcomes as appropriate to report equity breakdowns. We will not be prescriptive about the number of the outcomes, as it will depend on the number of study design types and the nature of the project aims. We are asking for one way cross tabulations of each primary outcome by these equity-relevant variables, if appropriate for your research, together with the number of observations in each cell. If more detailed cross tabulations are appropriate for your proposed research, please include these as well. This request applies to both primary data collection studies and secondary analysis of routine data, and to causal inference studies as well as descriptive studies; however, if this is not possible due to data limitations then please explain. Due to sample size and other data limitations there may be difficult scientific and/or data security*** judgement calls to make about which breakdowns to report and whether to merge categories to increase counts in particular cells; we ask you to make these judgments yourself, bearing in mind our data curation aim of enabling future evidence synthesis work in pooling results from different studies. We also ask that researchers report breakdowns for the unadjusted as well as adjusted outcomes/effects, as appropriate.
We understand that research projects may employ different methodologies, and focus on different populations. Please explain how the variables and data collection methods chosen are appropriate to the methodologies used.
We ask that you please clearly identify in the research plan section of the application whether your application has a health inequalities component or not and detail the core set of health inequality breakdown data that will be collected, if applicable. Submission of the data collection will be a condition of the final report for all research with relevant methodologies regardless of whether the research has a health inequalities component that will need to be submitted to NIHR PRP when the grant has finished. This should only take a few sentences within the research plan section.
* Table below uses the nine regions in England, further regions can be used if using the UK as the study population. Please report region breakdown for large samples in nationally representative descriptive studies. There is no need to report this for small sample studies, for sub-national studies, or for quasi-experimental studies where it would require time-consuming re-estimation.
** White, Mixed/ Multiple ethnic groups, Asian/ Asian British, Black/ African/ Caribbean/ Black British, Other ethnic group. If the sample size is small then it is fine to report only some of the requested equity breakdowns and to merge some of the sub-groups as appropriate.
*** For guidance on how to handle data security concerns in reporting of sensitive data please see ONS guidance.
Example data table for submission at the end of the funded research project
(N.B. If there is more than one main outcome then you will require more tables and if you adjust your outcome then you will need two tables for the adjusted outcome and unadjusted outcome. For other methodologies, variable vs number of observations may be more appropriate to record participant data). This table is for an example only. It does not contain sub variables and does not illustrate any preference for certain variables, as these will be dependent on the proposed research.
Variable |
Outcome (an appropriate average for this subgroup, usually the mean) |
Number of observations |
Additional information about variation if appropriate, e.g. range, standard deviation | |
|---|---|---|---|---|
Age |
- | - | - | |
Sex |
- | - | - | |
Gender |
- | - | - | |
Disability |
- | - | - | |
Ethnic Group |
- | - | - | |
IMD Group |
- | - | - | |
Region |
- | - | - | |
Appendix B: Health Inequalities in NIHR PRP Research Q&A Event
This event will take place on Monday, 19 September 2022 from 2:00 - 3:00pm. There will be a discussion from the NIHR PRP, the Department of Health and Social Care and other panellists followed by the opportunity for a Q&A session to help applicants navigate this new request. Please register for the event using the google registration form for the event. Any questions that are not answered during the session will be anonymously answered and published in a FAQ document on the health inequalities webpage.