
Diverse and innovative research approaches are needed to tackle complex health and social care challenges. NIHR Programme Grants for Applied Research (PGfAR) is seeking to increase the novelty and ambition of research designs awarded funding. We have funded a number of awards in recent competitions that have risen to the challenge, including this case study in which an innovative research design is being applied to investigate what happens when children and young people with painful joints and muscles visit their doctor, and how we can improve their understanding and care.
Programme Details
Title: Addressing Child and Adolescent Musculoskeletal Pain: the CAM-Pain Programme
Lead Researcher: Prof Kate Dunn
Institution: NHS North Staffordshire CCG and Keele University
Funding: £1,499,825.00
Benefits to patients and the NHS
Pains in the feet, knees or back are common in children, and experiencing such pain in childhood or adolescence appears to increase the risk of adult musculoskeletal pain. A leading cause of disability across the world, multinational prevalence studies have found that 60% of 9 year-olds reported pain in the surveyed month, and up to 44% of children and adolescents report chronic pain. Back and neck pain is among the top 10 causes of disability globally among 10-14 year-olds, rising to fourth place among 15-19 year-olds, before becoming the main cause among 25-29 year-olds. Despite this, there is hardly any research about childhood musculoskeletal pain and we know very little about:
• children who visit the doctor.
• who gets better and who does not.
• what treatments are given.
• how children or parents feel.
Childhood pain episodes are windows-of-opportunity to empower children to learn new information, skills and adopt positive health and pain management behaviours. Intervening early to support children and adolescents to understand and self-manage pain may reduce impacts of, or prevent, musculoskeletal pain in childhood, adolescence and into adulthood.
Aims of the Programme
This programme aims to improve the understanding, self-management, impact and healthcare of early episodes of musculoskeletal pain in children and adolescents, from individual, family, clinician and policymaker perspectives.
Programme Design
This programme builds on previous related research conducted in other countries, and is structured around four interlinked work packages with overlapping timelines.
The research team will study existing anonymous medical records, collected nationally. They will work with children, parents and healthcare professionals, and review research and treatment guidelines to develop and plan roll-out of an information and support package for children (and parents) about musculoskeletal pain. The package of resources will then be tested and evaluated in doctors’ practices.
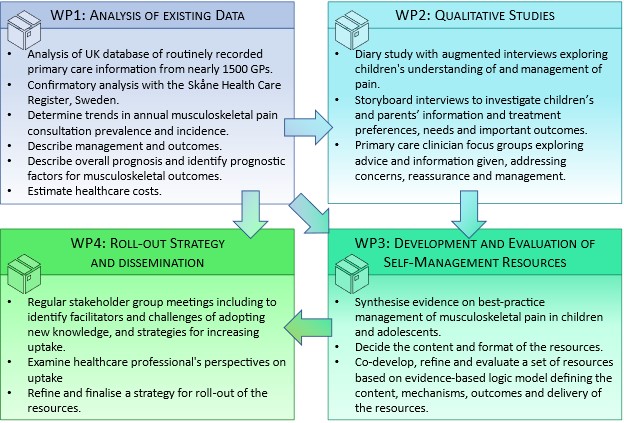
Work package 1 - Epidemiology, current management and healthcare costs of musculoskeletal pain in children and adolescents in primary care
This work package will produce data on prevalence, incidence, trends, management, prognosis, prognostic factors and healthcare costs for child and adolescent musculoskeletal pain.
Methods: Analysis of a UK database of routinely recorded primary care information from nearly 1500 general practices including around 1 million children and young people, with confirmatory analysis in the Skåne Health Care Register, Sweden. This analysis will:
- determine trends in annual musculoskeletal pain consultation prevalence and incidence (2005-2020).
- describe management and outcomes including repeated consultations, prescriptions and referrals.
- describe overall prognosis and identify prognostic factors for musculoskeletal outcomes.
- estimate healthcare costs per child or adolescent and overall health service costs.
Work package 2 - Determine views and experiences regarding child and adolescent musculoskeletal pain, pain management, treatment preferences and priorities, information preferences and needs, and important clinical and patient outcomes.
This work package will explore the views and experiences of primary care musculoskeletal pain management.
Methods:
- Diary study with augmented interviews exploring children’s and adolescents’ understanding and management of pain.
- Storyboard interviews with children and adolescents and parents to investigate information and treatment preferences, needs and important outcomes.
- Primary care clinician focus groups exploring advice and information given, addressing concerns, reassurance and management.
Work package 3 - Developing and testing information and self-management resources for musculoskeletal pain in children and adolescents
This work package will develop and evaluate new information and self-management resources.
Methods:
- Synthesise evidence on best-practice management of musculoskeletal pain in children and adolescents.
- Consensus group meetings to decide the content and format of the resources.
- Findings from WP1-3 triangulated to develop an evidence-based logic model outlining the content, mechanisms, outcomes and delivery of the resources.
- Meetings and interviews with children and adolescents, parents and clinicians to co-develop and refine the information and self-management resources.
- Evaluate use of the information and self-management resources in general practice.
Work package 4 - Explore and plan roll-out of the information and self-management resources
This work package will develop and finalise a full strategy for roll-out of the information and self-management resources.
Methods:
- Regular stakeholder group meetings including children and adolescents, parents, clinicians, researchers, and policy makers to identify facilitators and challenges of adopting new knowledge, and strategies for increasing uptake.
- Examine healthcare professionals’ perspectives on uptake of the information and self-management resources in general practice, and plan broader roll-out.
- Refine and finalise a strategy for roll-out of the resources.
Why was this programme design chosen?
We based our decisions for the study designs used within the programme on the most suitable ways to achieve the aims of the programme. We did not feel that an RCT was appropriate for achieving our aims. There is very little research published, and no treatment guidelines, on musculoskeletal pain in children and adolescents in primary care (the setting in which the research is based). There are currently no evidence-based materials available for clinicians to give to children and young people seeking primary care with musculoskeletal pain. Comparing an evidence-based, low risk, no-cost set of resources (that were co-developed with children, young people, parents and healthcare professionals), to usual practice (i.e. no materials given out) did not seem appropriate, ethical or feasible. We felt that clinicians would be unlikely to feel much uncertainty between the two choices.
We have put a lot of effort into designing a programme that will have outputs with potential to influence practitioners, policy makers, commissioners and the public, most importantly by involving people with those different viewpoints throughout the programme of research.