
15 September 2023 update: Our Theory of Change for NIHR Global Health Research Groups has recently been updated. Groups 5 applicants, please refer to our new Global Health Research (GHR) Groups Programme Theory of Change. A new theory of change for NIHR Global Health Research Units will be published soon.
Aim
NIHR has developed this Theory of Change to illustrate to potential applicants to the NIHR Global Health Research Units Call 2 and NIHR Global Health Research Groups Call 3 a selection of example activities, outputs, and outcomes reflecting the core aims, objectives, and funding criteria of the Units and Groups. We would emphasise that it is intended merely as a visual representation of the programmes’ core principles and ambitions, drawing on scoping work and discussions that have informed the initial commissioning. Thus we would encourage applicants to think creatively and broadly in how they interpret and further build on the Theory of Change, in terms of how concepts apply in their own local contexts.
NIHR intends and expects this Theory of Change to be updated and evolve as part of activities linked to successful Units’ and Groups’ own strategies to deliver wider impacts, and monitoring, learning and evaluation plans - and welcomes prospective applicants’ feedback on how the principles and ambitions set out in this guidance relate to their own ambitions, contexts and experiences. Please email nihrglobalhealth@nihr.ac.uk with any feedback.
Process
This Theory of Change has been developed collaboratively through a series of workshops with key stakeholders including the Department of Health and Social Care (DHSC)’s Global Health Research team and advisory board, NIHR Coordinating Centres, other strategic delivery partners and award holders.
Theory of Change
* Research-enabling staff refers to research managers, finance and admin staff.
** Equitable research partnerships and networks is defined in line with Sustainable Development Goal (SDG) 17: ‘Enhance North-South, South-South and triangular regional and international cooperation on and access to science, technology and innovation and enhance knowledge sharing on mutually agreed terms.
***A research ecosystem refers to researchers and their outputs, research institutions, funders, policy makers who use the research to inform policy, communication specialists who share findings with the public, and private sector companies who develop products and employ researchers.
The Theory of Change diagram for NIHR Global Health Research Units and NIHR Global Health Research Groups is a nested theory of change, which should be viewed as a sub-set of the overarching Global Health Research Portfolio Theory of Change.
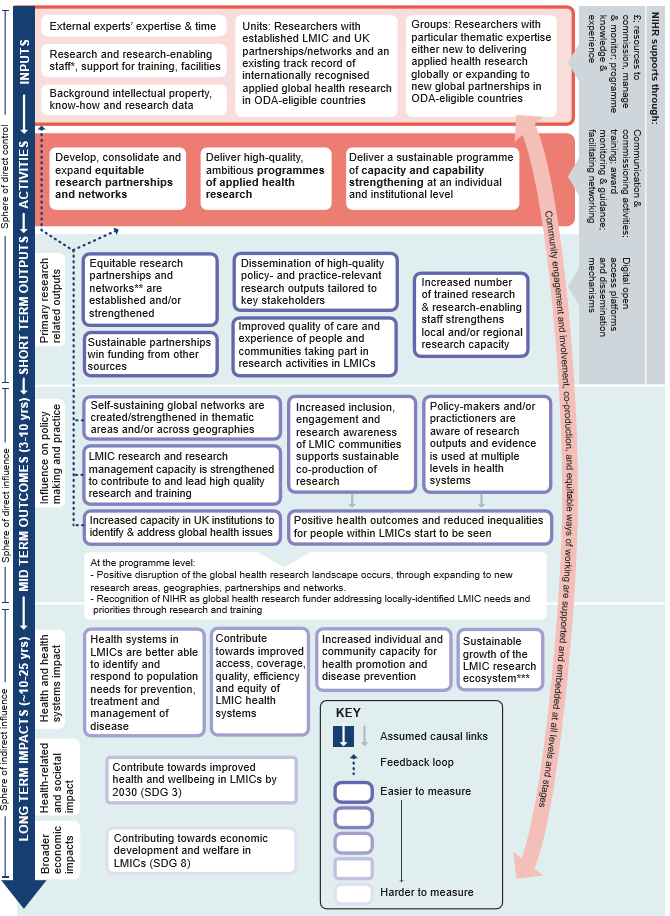
This Theory of Change demonstrates the inputs, activities, outputs, outcomes and impacts that reflect the core aims, objectives, and funding criteria of the Global Health Research Units and Groups. It is a visual representation of the programme’s core principles and ambitions, shown in a series of logical steps.
The Theory of Change shows the inputs that are required for the programme to work effectively and the activities that take place using these inputs. It also shows how these inputs and activities are expected to result in short-term outputs, mid-term outcomes and long-term impacts, which occur at various points in time.
White arrows on blue background indicate the assumed causal flow starting with how the resources deployed (inputs) to enable activities to take place lead to a set of expected results (outputs) in the short-term, which feed into changes (outcomes) in the medium-term and finally culminate in long-term impacts occurring after around 10-25 years. Inputs, activities and outputs are stages that are within the direct control of the NIHR Global Health Research Units and Groups, while the outcomes may be directly influenced (rather than controlled) and impacts only indirectly influenced. The impacts relate to the global needs that these programmes were designed to play a role in addressing. Moving from outputs to outcomes and impacts, they become harder to measure, which is represented by fading of the box frames.
Some significant reverse flows are expected, and these are indicated by broken blue lines from bottom to top (e.g. global networks are created as an outcome, which will likely feed into inputs in future research funding rounds). The role NIHR plays in supporting the Global Health Research Units and Groups is illustrated by the grey boxes on the right with arrows from right to left, which feed into the inputs, activities and outputs.
The diagram also shows the sphere of control that the NIHR Global Health Research Units and Groups programme might be expected to have. The programme has direct control over inputs, activities and short-term outputs, it can directly influence mid-term outcomes and it has an indirect influence on long-term impacts.
The first stage of the diagram focuses on the inputs for the successful working of the programme:
- the expertise and time of external experts in funding processes
- research staff and research-enabling staff, training and facilities of Units and Groups
- background intellectual property, know-how and research data that research teams bring to their awards.
In addition, Units bring inputs in terms of researchers with established low and middle income country (LMIC) and UK partnerships or networks and an existing track record of internationally recognised applied global health research in countries eligible for Official Development Assistance (ODA). Groups bring specific inputs in terms of researchers with thematic expertise who are either new to delivering applied health research globally or who are expanding to new global partnerships in ODA-eligible countries.
As a funder, the NIHR supports these inputs in terms of resources (money, knowledge and experience) to commission, fund, manage and monitor the programme.
These inputs then feed into the second stage consisting of the activities undertaken by Units and Groups using their inputs throughout the award period:
- develop, consolidate and/or expand equitable research partnerships and networks
- deliver high-quality, ambitious programmes of applied health research
- deliver a sustainable programme of capacity and capability strengthening at an individual and institutional level
At the funder level, NIHR supports these activities through its own activities around communication, commissioning, training (through the NIHR Academy), award monitoring/guidance and facilitating networking between teams.
There is an arrow indicating the causal flow linking the activities to the third stage – this consists of the intended short-term outputs, which are the tangible, measurable products, goods and services resulting from the activities. In the short term, the following outputs are expected, in line with activities:
- the establishment/strengthening of equitable and sustainable research partnerships and networks, able to win funding from other sources
- the dissemination of high-quality policy/practice-relevant research outputs tailored to key stakeholders
- an increased number of trained research and research-enabling staff to strengthen local and/or regional research capacity.
Moreover, even in the short-term, we hope to see an improved quality of care and experience of care among people and communities that directly take part in the research activities in LMICs.
As a funder, NIHR supports the generation of short-term outputs by providing digital open access platforms and dissemination mechanisms.
Moving onto the fourth stage (mid term outcomes), after around three to 10 years, we expect to see the following outcomes:
- an influence on policy making and practice, as policymakers and practitioners become aware of research outputs and evidence and use these at multiple levels of the health system so that we begin to see positive health outcomes and reduced inequalities for people and communities in LMICs
- the increased inclusion, engagement and research awareness of LMIC communities to support the sustainable co-production of research
- self-sustaining global networks which are created or strengthened in thematic areas or across geographies
- strengthened LMIC research and research management capacity for contributing to, and leading, high quality research and training. The increase in capacity for identifying and addressing global health research issues should also be seen in UK institutions.
There are also some mid-term outcomes that NIHR would expect to see at the funder level. These include the positive disruption of the global health research landscape, with the Global Health Research Units and Groups cohort expanding to new research areas, geographies, partnerships and networks. In addition, we would like to see increasing recognition of the NIHR as a global health researcher funder, which addresses locally identified LMIC needs and priorities through research and training.
The final stage of the diagram shows long-term impacts. In the long term (approximately 10-25 years), the changes in policy, practice and behaviour are expected to contribute towards strengthened health systems, increased individual and community capacity for health promotion and disease prevention, and the sustainable growth of the LMIC research ecosystem. Somewhat harder to measure, but something NIHR still expects to have an impact upon, is economic development and welfare in LMICs. These impacts tie into Sustainable Development Goals (SDG), notably SDG 3 (“ensure healthy lives and promote wellbeing for all at all ages”), SDG 8 (“promote sustained, inclusive and sustainable economic growth, full and productive employment and decent work for all”) and SDG 17 (“strengthen the means of implementation and revitalizing the global partnership for sustainable development”).
The diagram also shows some reverse flows. So, for instance, the global health research networks which are created or strengthened as a mid-term outcome will feed back into inputs and activities in future funding programmes.
Finally, community engagement and involvement, co-production and equitable ways of working are supported and embedded in all activities and at all stages of the model.
Increasingly, as the theory moves from the top towards the bottom of the diagram, the theory of change relies on set assumptions around the causal links. Where assumptions do not hold true, there is a risk that these will cause a break in the causal links, which could undermine the achievement of the intended outcomes and impacts. NIHR will monitor the assumptions and risks to test if any mitigation is required.
These assumptions are likely to play out differently over time and space; LMIC settings are not homogenous:
Inputs:
- UK-LMIC partnerships can successfully and effectively deliver global health research
- Applications, submitted and funded, are based on LMIC-led and needs-driven priorities for sustainable research solutions in support of SDGs
- Applicants have the knowledge and networks for CEI during the pre-award stage to co-produce proposals
- Applicants are able to bring the necessary input resources
Activities:
- Research areas continue to reflect LMIC-led and needs-driven priorities
- Activities are efficient and contribute to value for money
- Units and Groups are able to mobilise, expand and strengthen partnerships and networks
- Units and Groups are able to achieve equity and collaboration at all levels of working, including at the pre-award stage, and are South-South as well as North-South
- Units and Groups have the ability to effectively identify and engage policy-makers
- Active CEI is maintained throughout the process, including in the generation of priorities for research
- NIHR funding and monitoring activities support equitable ways of working
- NIHR communication activities are sustained throughout and reach intended audiences
Outputs:
- Research outputs consider access, coverage, quality, efficiency, equity
- NIHR award level dissemination platform/mechanisms are recognised and used
- Partnerships and networks established are sustainable and able to attract funding from other sources
- Learning and translation between partners and settings is accepted and acted upon
Outcomes:
- Policy-makers/practitioners have the resources and the political will and ability to understand and use research findings
- Institutional capacity for research is supported within the LMIC environment and trainees are retained within the LMIC research ecosystem to support future sustainability
- Locally-driven work packages have potential for wider geographic generalisability
Risks:
- Researchers do not have skills, knowledge and networks to disseminate findings effectively to policy-makers and practitioners
- External influences e.g. social, political, economic, environmental, technological, legal, demographic, cultural context hamper the research process or the uptake of research evidence.
Next steps
NIHR intends to regularly review and update this Theory of Change as evidence is gathered through the lifetime of the Global Health Research Units and Groups portfolio. The Theory of Change will form the basis of ongoing and future monitoring and evaluation activities.