
Diverse and innovative research approaches are needed to tackle complex health and social care challenges. NIHR Programme Grants for Applied Research (PGfAR) is seeking to increase the novelty and ambition of research designs awarded funding. We have funded a number of awards in recent competitions that have risen to the challenge, including this case study.
Programme details
Title: Personalised Care for Early Psychosis
Researcher: Dr Paul French
Institution: Pennine Care NHS Foundation Trust
Funding: £1,015,362.00
Benefits to patients and the NHS
Evidence from this research will inform national commissioning of Early Intervention in Psychosis (EIP) services. The generation of a large, linked dataset will create opportunities for building further research capacity and collaborations.
Aims of the programme
- To understand current Early Intervention in Psychosis (EIP) provision
- To investigate the impact of the duration of EIP treatment on health outcomes
- To estimate the cost-effectiveness of flexible, needs assessed EIP services
- To develop evidence-based guidance to guide clinical decision making and commissioning
Programme design
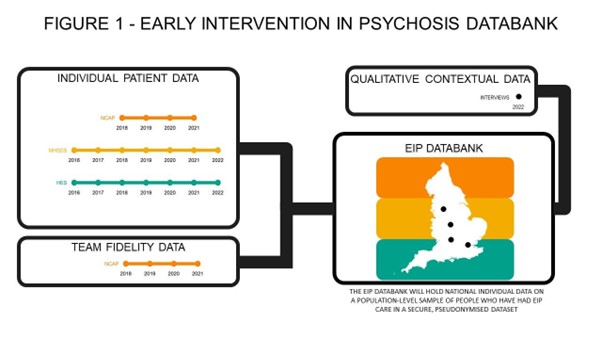
The programme is structured around 4 interlinked work packages (WP). WP1 will use mixed methods to measure and understand variability in duration and delivery of EIP treatments. Figure 1 below demonstrates how data from different sources will feed into the EIP Databank. This work will inform the causal modelling and health economic analyses of WP2 and WP3. The policy and engagement work (WP4) will run throughout the programme to ensure key stakeholders can inform all aspects of the research.
Work package 1: How are decision about duration of treatment for EIP made?
This work package aims to understand the contributing factors to the length of EIP treatment received. These may be related to individual service users factors e.g. demographics, social factors e.g. employment and housing, clinical judgement and service delivery.
Methods: WP1 will use both qualitative and quantitative approaches to define current decision-making about when to discharge people from EIP. Qualitative contextual data will be gathered via interviews with service users, family carers and stakeholders will be used to describe and understand the variation in service provision in EIP services across England. Individual patient data from National Clinical Audit of Psychosis (NCAP), Mental Health Services Dataset (MHSDS) and Hospital Episode Statistics (HES) and Team Fidelity Data via NCAP will be used to conduct a quantitative analysis to identify individual variations to EIP treatments received and duration of treatment.
Work package 2: The impact of the duration of EIP treatment on health and social outcomes
A mixed-methods approach will be used to determine whether the duration of EIP care is causally associated with outcomes. The main outcome of interest will be relapse after EIP treatment has ended.
Methods: Inpatient admission data including number of days spent in hospital as well as information on acute hospital attendance, new physical health diagnosis and mortality will be collected alongside comprehensive qualitative case studies.
Work package 3: The economic consequences of moving to a needs-based, personalised duration of EIP service
This WP will focus on the economic impact of moving away from a time-limited EIP service. It is argued that prolonging EIP, in those who need it, will substantially improve health outcomes and reduce avoidable health service costs.
Method: The cost-effectiveness of moving from a time-limited to a flexible EIP service will be estimated, through approximating the health outcomes and healthcare resource use of patients in the short and medium-term for both strategies. Resource use will be converted into national unit costs and the average cost of EIP services per year will be calculated. A psychosis model will then be used to estimate lifetime health service costs and Quality Adjusted Life Years (QALYS). Lastly, the level of need and total resources needed to provide personalised EIP to everyone in need in England will be calculated.
Work Package 4: Laying the pathway to policy of a needs-based EIP approach
EIP services will remain a priority for mental health services over the next decade. This WP will run parallel to the other research programme WPs. Key stakeholders across the public, health services and government will be engaged to understand the higher-level barriers to a more personalised model of case and provide a link between stakeholders and researchers. The aim of this WP is to ensure this programme makes a lasting difference to policy and practice in the UK and internationally.
Method: A series of workshops and roundtable events will be held with leaders from local systems across the country. Participants will include leaders from NHS mental health trusts, integrated Care Systems (ICS), local authorities, voluntary and community organisations and experts by experience. These events will give an insight into the current issues and pressures they are facing as well as be an opportunity to share emerging findings from the programme.
Why was this programme design chosen?
Our proposal is important from an NHS service perspective. The Five-Year Forward View for Mental Health 2016-2021 set the ambition that by 2021 at least 60% of people with a first episode psychosis would start treatment with a NICE-recommended package of care with a specialist early intervention in psychosis service within two weeks of referral. Subsequently, the NHS Long Term Plan has reconfirmed the NHS’s commitment to the EIP access and waiting time standard, with this commitment sitting within wider transformation work to improve England’s community mental health services and crisis services.
Alongside this transformation work, NHS and National Institute for Clinical Excellence (NICE) has recently published guidance on rehabilitation for adults with complex psychosis. It highlighted that regardless of the current successful approach by EIP, a number of people attain only a limited recovery from psychotic related symptoms and functional impairments, indicating a need to better understand who may require more long-term care alongside considering the possibility of rehabilitation. The new NICE guidelines highlight that a 2 -3 year window of interventions is not a panacea for everyone and some people may well benefit from an extended period of time in EIP to consolidate what has been achieved.
NHS England identified the question of whether extending EIP improves and maintains good outcomes as the only mental health research priority requiring ‘immediate activity’ in their 2018 research needs assessment. The research team was successful in being awarded an NIHR HTA research grant to answer this question through a Randomised Controlled Trial (NIHR129501), however, excess treatment costs were thought by NHS England to be prohibitive and meant the trial was unable to proceed. The issue remained a vital question for the NHS but costs of conducting a trial meant that another methodology was required. Therefore, the team developed the programme of research described above as an alternative strategy to answer this important question which addresses a key priority for patients, families and the NHS.