
This document sets out the call specification for the NIHR Invention for Innovation (i4i) OLS Cancer Mission: Early Cancer Diagnosis Clinical Validation and Evaluation Call.
The NIHR i4i Programme, in collaboration with the Office for Life Sciences (OLS), invites applications to the Cancer Mission: Early Cancer Diagnosis Clinical Validation and Evaluation Call. Proposals must demonstrate how the selected innovation will increase the proportion of cancers diagnosed at stages 1 and 2. Proposals aiming to directly address health inequalities in stage of cancer diagnosis are particularly sought.
The Cancer Mission: Early Cancer Diagnosis Clinical Validation and Evaluation Call is a one-stage call inviting applications for projects up to 36 months in duration, with no upper funding limit.
The call will be open to organisations which are UK legal entities, that have an innovative solution with the potential to increase the proportion of cancers diagnosed at stages 1 and 2. This call is open to small/medium commercial entities, NHS and Third Sector Service Providers, charitable organisations, local government bodies, as well as universities and research institutions.
Introduction
The NIHR Invention for Innovation (i4i) Programme, in collaboration with the Office for Life Sciences (OLS), invites applications for a £12m funding call aimed at the clinical validation (assessing that the approach does what it is intended to do, accurately and reproducibly in real people in a clinical setting) and evaluation (assessing whether the approach informs clinical practice in the intended way and/or has clinical impact on patient outcomes) of innovations with the potential to increase the early detection and diagnosis of cancer. We particularly welcome proposals that aim to directly address inequalities in stage of cancer diagnosis. Proposals may focus on a single cancer or target multiple cancer sites.
The Life Sciences Vision, published in July 2021, co-developed by the Government, the NHS and the Sector set out our shared ambition to make the UK a Life Science Superpower.[1] The Vision outlined how, through building on the UK’s existing strengths and potential, and harnessing the lessons of the Life Science response to COVID-19, there was an opportunity to significantly enhance the UK’s competitiveness and drive value creation for the public and private sectors. The Vision set out ambitions for healthcare missions – selected as disease areas and conditions that drive significant mortality and morbidity in the UK and globally.
The Cancer Mission is being led by OLS and aims to make the UK a leading testbed for oncology innovation by accelerating the development and commercialisation of a new generation of cancer diagnostics and therapeutics, allowing patients to be diagnosed earlier and offered therapies specifically designed to target their cancer. At the end of 2022, the UK Government committed £22.5m to deliver the Cancer Mission.[2] This £12m funding call forms one element of the Mission.
The call is open to organisations which are a UK legal entity, including small/medium commercial entities, NHS and Third Sector Service Providers, charitable organisations and local government bodies, as well as universities and research institutions. Organisations can be based anywhere in the UK, and the proposed research must show potential, and be appropriate, for roll out and use in the UK. Applicants will be asked to evidence a future business development plan, including a strong implementation and commercial plan for the UK and NHS England.
Projects must partner with at least one NHS organisation to ensure delivery of the project in line with NHS clinical needs. Engagement with other organisations and groups in the cancer research infrastructure is encouraged. Further details of suggested collaborative engagement are provided below in the Entry Criteria section.
Support with research design and forging partnerships is available to all prospective applicants through the NIHR research support services, detailed below. All prospective applicants are encouraged to engage with these services at the earliest opportunity.
Background
Cancer is one of the leading causes of morbidity and mortality in the UK, responsible for 25% of all UK deaths in 2021.[3] There are approximately 375,000 new cancer cases and 167,000 cancer deaths each year in the UK.[4] One in two people born after 1960 are expected to be diagnosed with cancer in their lifetime.[5] The UK has made substantial progress to improve cancer survival over the last decades, with one year survival for patients (in England) diagnosed in 2019 at 74.6%, over 10 percentage points higher than in 2004 (64.4%).[6] Early cancer diagnosis is critical to driving further improvements.
Across the UK, strategies have been developed to improve cancer outcomes, with a focus on increasing the proportion of cancers diagnosed in the early stages of the disease.[7][8][9][10] Earlier diagnosis of cancer is critical to improving cancer outcomes across the population as it increases the likelihood of a patient’s condition being more effectively treated and managed.[11] A multitude of actions will drive earlier diagnosis of cancers, but research, innovation and technologies will play a key role to support faster, more efficient, and earlier cancer diagnosis.[12] Technological advances are driving a step change in early diagnosis – new tests have the potential to screen for cancer by detecting multiple types of asymptomatic cancers from a single blood sample, novel diagnostics can identify early signs of cancer at earlier stages with more efficiency, and artificial intelligence (AI) solutions enable more rapid analysis of health data, to support case finding and earlier, faster and more efficient diagnosis.
Early diagnosis rates vary between different cancer sites (see the Case-mix adjusted percentage of cancers diagnosed at stages 1 and 2 in England, 2020 for reference). For example, cancer sites such as oesophageal, pancreatic and non-Hodgkins's lymphoma have particularly poor early diagnosis rates. Other cancer sites, such as lung and colorectal cancer have a slightly higher proportion of cancers diagnosed at stage 1 and 2, though the overall number of cases means they are still important areas for intervention.
Whilst cancer is a burden on the whole population, there are inequalities in stage of cancer diagnosis for different communities. In England, the NHS Long Term Plan [13] and Core20PLUS5 [14] approach to reducing healthcare inequalities highlight stage of cancer diagnosis as a priority area. The NHS Long Term Plan set an ambition to diagnose 75% of staged cancers at stage 1 and 2 by 2028 – an increase from 55% in 2019.[15] Those in the most deprived communities are less likely to be diagnosed at the earliest stages of cancer than those in the least deprived areas. For example, in England there is a 7-percentage point difference in early diagnosis rates between the 20% most deprived areas and 20% least deprived areas.[16] Similar patterns are seen in Scotland, with approximately 20% poorer uptake of cancer screening in the most deprived areas compared to the least deprived.[17] Further evidence reported that people with learning disabilities are 45% less likely to be screened for cancer compared to their counterparts without learning disabilities.[18] Incidence of some cancers also varies between different ethnic groups, for example myeloma and stomach cancer are more common in black men than men from other ethnic groups. Biological differences in cancer aetiology between groups can present challenges for universal effectiveness of early detection approaches.
The launch of the Cancer Mission: Early Cancer Diagnosis Clinical Validation and Evaluation Call presents up to £12.2m to support the clinical validation and evaluation of innovations with the potential to increase the proportion of cancers diagnosed at earlier stages. The call invites applications for up to 36-months with no upper funding limit. Applications that address health inequalities in early cancer diagnosis are particularly welcomed.
Scope and Aims
The aim of the call is to support the clinical validation and evaluation of breakthrough technologies that can increase the proportion of cancers which are detected earlier in the disease course and/or target health inequalities in stage of cancer diagnosis. Funding will be deployed to facilitate the generation of evidence on safety, test performance characteristics, clinical efficacy and/or effectiveness that can support regulatory approvals requirements and subsequent clinical implementation or implementation research.
The expected objectives of this investment are to:
- Improve patient outcomes – innovative technologies to support earlier, more efficient and faster diagnosis. This is an area of unmet healthcare need (as set out above). This will increase the effectiveness of an existing public service and improve cancer survival.
- Reduce the economic cost of healthcare through earlier diagnosis by utilising innovative technologies to detect cancer earlier and reduce the proportion of cases requiring the expensive, longer-term therapy that is necessary for treating late-stage disease.
- Reduce health inequalities in cancer detection and diagnosis by harnessing innovations that will reduce inequalities in early diagnosis rates, tackling a contributor of the socio-economic life expectancy gap by decreasing inequalities in cancer outcomes.
- Position the NHS as a strong innovation partner able to drive and inform the development of innovative diagnostics and services by testing innovative products and care models to support wider uptake.
- Support the commercialisation of innovative life sciences technologies in the UK and stimulate wider investment into R&D from the private, charity and philanthropic sectors.
- Improve understanding and research into oncology and supporting the UK’s position as a leader in cancer research – the outputs created through R&D will stimulate the development of a rich evidence base for the further development of new treatments and services. In addition, R&D funding may support further training opportunities to ensure that the sector has right skills to harness the potential of new technologies in the future.
Areas in Scope
Types of eligible innovations include, but are not limited to, medical devices, in vitro diagnostics, NICE classified Tier C digital health solutions, software, artificial intelligence, behavioural interventions and new models of care.
Applicants may wish to consider the following (non-exclusive) potential solutions to improving early diagnosis of cancer:
- Identifying and testing asymptomatic patients who are most at risk. This includes innovations that:
- Proactively case find and/or risk stratify populations for whom there is no current screening programme.
- Use risk stratification to more effectively target, improve uptake/adherence, or reduce unwarranted variation in existing screening programmes.
- Screen asymptomatic individuals at risk.
- Encouraging early symptomatic patients to self-assess and present to primary care or other appropriate services. This includes innovations that:
- Proactively identify those with early signs and symptoms that put them at high risk.
- Improve awareness/vigilance of the signs and symptoms of cancer (including non-specific symptoms), particularly for those cancers, or specific populations, where early presentation is still very low.
- Encourage patients to self-present, including in populations that typically under refer.
- Support ongoing engagement and completion of diagnostic pathways.Decision support and assessment of risk in early symptomatic patients presenting to primary care. This includes innovations that:
- Risk stratify patients or diagnose patients that present with less severe and non-specific symptoms.
- Support GP decision making and reduce unwarranted variation in referrals (to increase appropriate faster referral and early diagnosis rates, whilst being mindful of avoiding unnecessary referral and attendant cost).
- Identify and alert clinicians to changes in a patient’s presentation, behaviour or symptomatology, or repeated attendances, that warrant consideration.
- Detection/diagnostic technologies for use in referral contexts for patients with non- specific symptoms or under suspicion of particular cancers which lack optimal diagnostic pathways and approaches.
- Approaches to address existing inequalities in stage of cancer diagnosis between socioeconomic, geographic, demographic or other subpopulations. Applicants may find it helpful to refer to the Core20PLUS5 approach for further information on population groups.
Funding is available for validation and evaluation of the potential to detect and diagnose earlier, in an NHS setting, either directly in individuals or in samples/data taken from these.
This can include, but is not limited to, funding for:
- Validation of markers, technologies or approaches in clinical samples or patients.
- Evaluation of markers/tests/technologies/approaches in a clinical setting, intended to deliver evidence on performance characteristics (e.g., sensitivity, specificity, positive or negative predictive value), impact on stage of cancer diagnosis, impact on referral pathways and service demand.
- Clinical utility studies covering e.g., usability, tolerability and user acceptance.
- PPIE activities.
Though not limited to these approaches, this call could be suitable for:
- Innovations that have been already in use or clinically tested outside the UK, but that still require clinical validation and evaluation for cancer in the NHS settings.
- Repurposing of approaches from a cancer area to another (e.g., biomarkers well validated for different cancers, but needing more evidence in a new area; extend new pathways to other cancers, etc.),or from other therapeutic areas to cancer diagnosis and detection.
Entry Criteria
This call is open to both innovations that are approaching their first clinical human testing, as well as more mature products (which might have CE or UKCA mark) but need to generate further evidence before starting their real-world implementation, implementation research or confirmatory trials in the NHS.
Technology Readiness Levels (TRLs) are a way to describe the maturity of a particular technology. There are 10 TRLs; 1 being the earliest level of readiness, and 10 being a technology which is freely available and fully developed for the market. See diagram and definitions below. Innovations which are the subject of proposals to this funding competition must already be at a minimum TRL of 4 and have been validated in the laboratory/the appropriate setting. Innovations must have a prototype for human testing ready, or only a minimum amount of product development required.
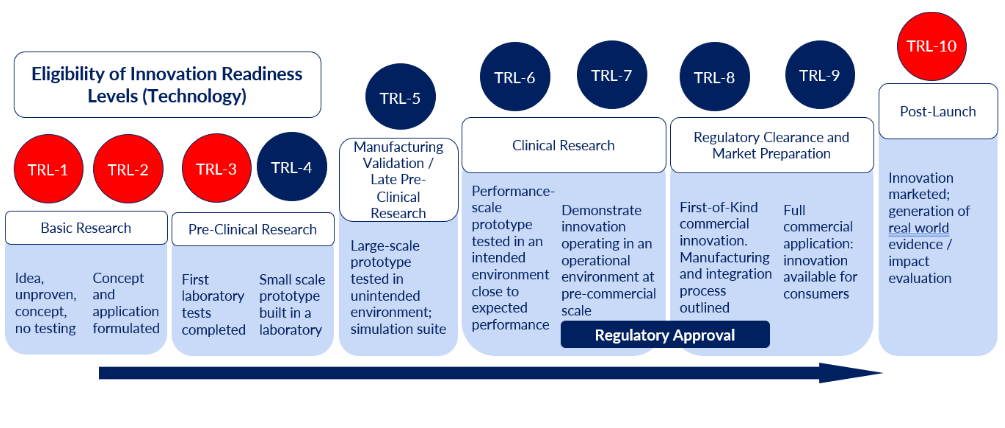
Figure 1: Entry Point Eligibility Schematic: Entry points in red are out of scope, those in blue are within scope. Please contact ols-cancer-mission@nihr.ac.uk to discuss eligibility.
Entry point Eligibility Schematic Description: Technology Readiness Levels (TRL)
- Not eligible (red)
- Basic Research
- TRL-1: Idea, unproven, concept, no testing
- TRL-2: Concept and application formulated
- Pre-Clinical Research
- TRL-3: First laboratory tests completed
- Post-Launch
- TRL-10: Innovation marketed; generation of real world evidence / impact evaluation.
- Basic Research
- Eligible (blue)
- Pre-Clinical Research
- TRL-4: Small scale prototype built in a laboratory
- Manufacturing Validation / Late Pre-Clinical Research
- TRL-5: Large-scale prototype tested in unintended environment; simulation suite
- Clinical Research
- TRL-6: Performance-scale prototype tested in an intended environment close to expected performance
- TRL-7: Demonstrate innovation operating in an operational environment at pre-commercial scale, gaining regulatory approval
- Regulatory Clearance and Market Preparation
- TRL-8: First-of-Kind commercial innovation. Manufacturing and integration process outlined, gaining regulatory approval
- TRL-9 :Full commercial application: innovation available for consumers
- Pre-Clinical Research
When submitting bids, applicants should provide:
- A strong evidence base proportionate to the level of readiness for the proposed markers/product (e.g., if the product has been validatedin laboratory settings, evidence of success must be demonstrated; if the product already has regulatory approval abroad/in another indication, evidence of this must be provided)
- Evidence of the clinical unmet need that the proposed approach will address.
- Evidence base and what has been done to date to demonstrate that the proposed markers/product can improve or has the potential to improve early cancer diagnosis and detection.
- Detailed description of the line of sight from the proposed research to impact on early detection/diagnosis and clinical benefit, including an articulation of the proposed next steps, should the study deliver the anticipated results.
- A detailed protocol for the study.
- Future business development plan, including a strong implementation and commercial plan for the UK and NHS.
- Details on how the proposed innovation will support equitable access to care and, where applicable, the potential the innovation has to improve current health disparities in stage of cancer diagnosis.
At least one NHS partner organisation must be included in the applicant team, to ensure the delivery of the project. Clinical partners can be based anywhere in the UK. Engagement with other organisations and bodies in the cancer research infrastructure is encouraged. Applicants may wish to engage with appropriate organisations and bodies, which may include:
- Cancer Alliances
- NIHR MedTech and In-Vitro Diagnostics Cooperatives (MICs)
- Experimental Cancer Medicine Centre (ECMC)
- Health Innovation Networks (previously known as Academic Health Science Networks)
- NHS Scotland Innovation Hubs
- NHS Research Scotland Cancer Network
- Wales Cancer Research Centre
- Wales Cancer Bank
- Welsh Cancer Network
- Wales Cancer Industry Forum
- Northern Ireland Cancer Trials Network
- Northern Ireland Trials Unit
- Northern Ireland Methodology Hub
- Northern Ireland Clinical Research Network
- Northern Ireland Clinical Research Facility
Expected Exit Points
The aim of the funding is facilitating the generation of evidence on safety, performance characteristics (sensitivity, specificity, PPV etc.), clinical efficacy and/or effectiveness to enable the completion of relevant regulatory approval and compliance required to support NHS implementation or progress to implementation research.
It is recognised that the exit point(s), i.e., the evidence and outputs generated by the end of the proposed research, will be different depending on the type of innovation and its level of maturity. Applicants will be asked to define the expected end point they intend to reach upon project completion. Examples of potential exit points include:
- Solid evidence of the performance of the test/marker approach (e.g., efficacy/effectiveness/sensitivity/specificity/PPV/NPV/impact on proportion of early/late-stage diagnosis).
- Evidence required to progress to larger-scale clinical trial/implementation research. N.B. Screening based innovations are expected to need further major trials.
- Innovation ready for the relevant regulatory approvals and compliance.
- Demonstration that the innovation can be applied to a new clinical pathway.
- For innovations fully validated outside the UK or in another indication, demonstration of their applicability to the NHS environment and/or the proposed indication.
- Evidence of health and financial impact associated with a health economics analysis (i.e., cost benefit analysis, budget impact model) to support future NHS adoption.
- Registration to HealthTech Connect / NHS Innovation Service.
- Insight into user acceptance through PPIE activity.
- Where applicable, demonstration of a signal that the innovation has the potential to impact inequalities in stage of cancer diagnosis.
- Business plan developed and clear route to approval and market access identified, including plan for generation of any further evidence required to support implementation.
Areas out of Scope
Projects that are excluded from this call include:
- Therapeutics, including vaccines or cell/gene therapies.
- Apps concerning general wellness and/or wellbeing, which are not specifically concerned with cancer symptom recognition and reporting.
- Digital Health Technologies in Tiers A and B.
- Early-stage research and discovery science.
- Innovations in the ideation or creation stage.
- Innovations that have not demonstrated proof of concept e.g., that have not demonstrated the ability to distinguish early cancer from normal tissue in limited numbers of human samples, or have not been shown in limited numbers of participants to affect the desired behaviour change.
- Innovations with limited or no impact on early diagnosis rates – e.g., focused on diagnostic efficiency rather increasing the proportion of cases diagnosed early.
- Innovations requiring further substantial product development iterations before starting the clinical testing (i.e., product development activities).
- Products that have shown proven efficacy or clinical effectiveness or are already used in standard routine care in the UK health system for the cancer(s) which is the focus of the proposal. NB. Products that are repurposed from one cancer to another and meet the eligibility criteria above remain in scope.
Call Details
Applicant Eligibility
Applicants are welcome from:
- Organisations which are a UK legal entity and include Higher Education Institutions (HEI), including universities and research institutes.
- NHS and social care service providers, including Trusts, primary care and community care providers and tertiary care centres.
- Small and Medium Enterprises (SMEs with a staff headcount no greater than 250 and an annual turnover no greater than €50 million, including start-up or spin-out companies).
- Not-for-profit organisations, including charities and Community Interest Companies.
Specialist services or expertise may be brought into the team through consultancy or sub-contract arrangements with appropriate justification. Collaborators and sub-contractors may be based outside of the UK if the required expertise or service cannot be reasonably contracted from within the UK. Involvement of international companies as subcontractor and/or collaborator, if working with a lead UK partner, are welcomed.
Applicants must review the NIHR standard research contract before application submission and agree in principle with its core terms and conditions as they are non-negotiable.
Applicant organisations can be based anywhere in the UK, and the proposed research must take place in the UK and show potential, and be appropriate, for roll out across the UK.
To support the growth of innovators in this field, applications from early career researchers and innovators are particularly welcomed. They can apply as either the lead or joint-lead applicant together with a senior colleague fulfilling the other role.
Consultation with individuals who have current or lived experience is expected.
Multidisciplinary project teams, involving relevant collaborations between technology developers, data scientists and clinical staff, are particularly welcome. The lead organisation should be best placed among the project parties, to lead the research, and either own or have full access to the background IP.
Budget and Duration
The call encourages proposals putting forward innovative solutions. To support this, there is no upper funding limit. Proposed projects may be of up to 36 months in duration.
We would expect the majority of applications to request up to £1.5m funding, however applicants are discouraged from compromising their ideas to meet this guideline, and applications will be considered on the overall merit and value for money they provide. Proposals may request smaller or larger funding amounts that reflect the scope and duration of the proposed project. Each proposal will be judged on its merits and value for money.
NIHR funding covers 100% costs for commercial entities, not-for-profit organisations, local government bodies, and primary care providers: 100% of the direct research costs for NHS service providers, and 80% FEC for higher education institutions.
Support for Applicants and Awardees
Support with research design and forging partnerships is available to all prospective applicants through the NIHR research support services, detailed below. All prospective applicants are encouraged to engage with these services at the earliest opportunity.
- NIHR's Research Support Service - support on all aspects of developing and writing a funding application. *
- NIHR's Business Development Team - help with finding and making great partnerships to strengthen your work.
- NIHR Medtech and In vitro diagnostics Co-operatives (MICs) - can help to build a multi-disciplinary team to work collaboratively and ensure the right generation of evidence to support adoption in the NHS.
If you are considering applying and you are new to research or are not from a research institution, please do contact the appropriate NIHR research support services for free advice and support in finding potential research partners. This support is also available for experienced researchers, free of charge.
* Please note that the RSS service is only available to applicants based in England. Applicants with a project partner based in England are able to access the service, but if you are based in the UK but outside of England and are not partnered with an organisation based in England you may wish to explore the below services. The NIHR Business Development Team is available to all UK based applicants, and you may wish to contact them in seeking a partner based in England.
Other organisations that may be able to support projects include:
- Applicants from Scotland may access NHS Scotland Innovation Hubs and/or NHS Research Scotland Cancer Network.
- Applicants form Northern Ireland may access The Northern Ireland Clinical Research Network.
- Applicants from Wales may access Health and Care Research Wales and/or Wales Cancer Industry Forum.
Key dates and Contacts
- Launch event: 6 October 13:00 (launch event recording)
- Q&A Session: 6 November 15:00 (registration page)
- Launch: 24 October 2023, 13:00
- Deadline for submission of applications: 12 December 2023, 13:00
- Assessment & Shortlisting: December 2023/January 2024
- Peer review (if shortlisted): Mid-February 2024
- Interview Committee: Mid April 2024
- Projects start: July 2024
- Committee Members
For any enquiries email: ols-cancer-mission@nihr.ac.uk
References
- Gov.uk - Policy paper Life Sciences Vision
- Gov.uk - Press release Government to use Vaccine Taskforce model to tackle health challenges
- Cancer Research UK - Cancer mortality for all cancers combined
- Cancer Research UK - Cancer Statistics for the UK
- Cancer Research UK - Cancer Statistics for the UK: Cancer Risk
- NHS Digital - Cancer survival: Index for Clinical Commissioning Groups, 2004 to 2019
- NHS Long Term Plan
- Gov.wales - Policy And Strategy: The quality statement for cancer
- Gov.scot - Publication - Strategy/plan: Cancer strategy 2023 to 2033
- Health-ni.gov - A Cancer Strategy for Northern Ireland 2022-2032
- NHS Long Term Plan
- Cancer Research UK - Early Detection and Diagnosis of Cancer Roadmap
- NHS Long Term Plan
- NHS England - Core20PLUS5 (adults) - an approach to reducing healthcare inequalities
- NHS Digital - Case-mix adjusted percentage of cancers diagnosed at stages 1 and 2 in England, 2019
- NHS Digital - Case-mix adjusted percentage of cancers diagnosed at stages 1 and 2 in England, 2020
- Cancer Research UK - Cancer Research UK report highlights stark cancer inequalities across Scotland
- PLOS ONE - Access to Cancer Screening in People with Learning Disabilities in the UK: Cohort Study in the Health Improvement Network, a Primary Care Research Database