
Timetable and Budget
| Description | Deadline/Limit |
|---|---|
| Deadline for Stage 1 applications | 14 February 2023, 1pm |
| Notification of outcome of Stage 1 application | April 2023 |
| Deadline for Stage 2 application | 06 June 2023, 1pm |
| Notification of outcome of Stage 2 application | October - November 2023 |
| Project start | January 2024 |
| Project duration | 12 - 18 months |
| Budget | £400,000 per project |
Introduction
The National Institute for Health and Care Research (NIHR) Policy Research Programme (PRP) invites applications for a single research project to evaluate the impact of the Enhanced RECONNECT (ER) programme pilot sites and identify areas of learning and future development. Two ER pilot sites have had business cases approved and were established at the end of 2022.
The ER service is NHS England’s (NHSE) response to the management of high complexity and high-risk offenders, in respect of their health and health outcomes. The vision for ER is to provide an integrated approach to engage (reconnect) these individuals in their care. It is a psychologically led, trauma-informed service, with the ethos that staff need to “make every contact count”. The service offers interventions, structured support, advocacy and signposting. ER builds upon the RECONNECT programme (see Appendix F), launched in a number of regions across England in 2019, and provides an enhanced pathway of care for those whose needs were not fully supported by the RECONNECT service.
Release from prison can be a crisis point for many individuals due to disruption to care pathways resulting in individuals becoming vulnerable to health relapse. The health gains made in prison can be lost through lack of engagement with community healthcare services. For those individuals leaving prison, ER provides the opportunity to engage with community-based health and support services with the aim of reducing social exclusion and health-related offending behaviours. ER offers interventions, structured support, advocacy and signposting.
Using a trauma-informed, formulation-driven and person-centred approach, ER services will support individuals leaving prison to better understand and manage their risks, build upon their strengths, learn new skills and identify and break down barriers to accessing existing community-based services.The service will work in collaboration with partners to ensure these individuals get the healthcare support they need to support the reduction of their risk of reoffending, which must be related to a health need.
The ER model aims to engage three priority groups (Appendix B) and will work with people from 6 months prior to release until 12 months post release. It is anticipated that the majority of the ER cohort will fall within Priority Group 3, however; ER services should ensure that referrals from Priority Group 1 & 2 are prioritised on receipt.
The intention is that findings from the study can inform later amendments to the service specification, to ensure that it meets the needs of this vulnerable and highly complex population. The work will also inform any decision on whether to roll out the ER services more broadly.
Background
The National Drug Strategy for England emphasises the importance of ensuring prisoners stay engaged in treatment after release and we want to ensure that individuals leaving prison with drug addictions are able to access substance misuse services upon release. In addition, the ER service will support the Government’s National Suicide Prevention Strategy, which includes a number of actions to reduce suicides for people in contact with the criminal justice system, including rolling out the RECONNECT service.
The ER service will specifically work with individuals that have highly complex health needs (as described in Appendix E), who may pose a risk to the public and those who need longer term support to engage and remain engaged with community health and support services. ER aims to support those that do not meet the threshold or are unsuitable for other risk management and support intervention services, whilst working collaboratively with such services to ensure patients have access to the correct intervention or service.
The service will work to support the Crime and Justice Task Force, who have set the target of engaging 75% of prisoners with identified substance misuse into substance misuse services upon release, through the focus on high-risk individuals with complex health needs, such as substance misuse and mental health conditions. The research may also support the identification of issues to address in future policy, such as the national drug strategy, violence reduction, and counterterrorism, as well as inform collaborative partnership working with criminal justice system colleagues who support and engage with offenders identified as high risk with complex health needs.
The ER service is not designed to take the place of community-based services. However, it will support those high complexity and high-risk individuals to engage in community-based services. Any intervention that the ER Service provides will be with the express aim of increasing the individual’s capacity to engage successfully with existing community-based services.
This research is required to assess the ER pilot sites. Both sites will be following the ER service specification but will be set up and rolled out into differing models of service delivery. We would like to know how effective the ER pilot sites are in delivering the service outcomes, how this is affected by the delivery model chosen for the service and its benefits and limitations, and what barriers are affecting the pilot’s ability to support access to services.
The research should aim to evaluate the impact the ‘Team Around the Individual’ (TAI) (Appendix C) Model adopted by the ER service can have on the highest levels of complexity and those who experience marginalisation.
Research priorities
The specific research questions we would like answered are:
-
What are the benefits and limitations of the TAI Model when applied in the ER service for this cohort of serious offenders? For example, does the application of the TAI Model to the ER service lead to increased wellbeing?
-
Are there specific barriers for the group of individuals who are part of the Enhanced RECONNECT programme that prevent them from engaging with community healthcare services?
-
Are there gaps in provision of meeting the health needs of all types of serious offenders?
-
How effective are the pilot sites at delivering on the service outcomes? See below (bullet 14-15) for detail of how we would expect some of the outcomes to be measured.
-
Where possible we would expect the researchers to collect individual outcomes to inform the high-level programme outcomes, such as those below, that are included in the national specification.
For the ER programme, a successful outcome is defined as an individual leaving prison attending their first healthcare appointment in the community and their healthcare needs being met or the patient having remained engaged for 12 months after leaving prison. Another service outcome is a reduction in repeat offending and risk of harm to self and / or others and a reduction in self-inflicted death. This could be measured through the OASys risk score assessments which are conducted in prisons by HMPPS staff. OASys is an actuarial risk and needs assessment tool used by the prison and probation services in England and Wales. The risk score is based on perceptions of staff and a scoring key is used for this.
There are several service outcomes for individuals including, but not limited to, improvement in relationships with professionals, improved engagement with health and justice services and a reduction in health-related re-offending behaviours, which this research should seek to evaluate. It is acknowledged that use of the prevention of re-offending as a metric for these cohorts is unlikely because the service will not track individuals leaving prison post 12 months. Therefore, we expect that all measurable outcomes will be based on health needs. Further detail on high-level and individual outcomes can be found in Appendix D.
The research should include all pilot sites, to enable comparison of how the delivery model affects the outcome of the service.
In addition, we want to understand the experiences individual’s leaving prison have with the service and the barriers they face in engaging with community healthcare services.
A Health Needs Assessment (HNA) has been conducted to enable the collection and subsequent analysis of data on the demand and need for health services among the ER cohort. The focus for the HNA is on the healthcare of those persons leaving prison who have complex clinical needs and who pose a high risk of harm to the public. The HNA has been completed and this can be made available to researchers on request.
New Guidance on Health Inequalities data collection within NIHR PRP Research:
Health Inequalities is a high priority area within the Department of Health and Social Care and the NIHR and is often present in a majority of funded projects. We are now assessing all NIHR research proposals in relation to health inequalities. We are asking applicants to identify in their application whether or not there is a health inequalities component or theme and how this research hopes to impact health inequalities. We are also asking researchers to collect relevant data, if appropriate for the research. Our goal is to collect information on health inequalities in research and data relating to the main outcome(s) of the proposed research. Please clearly identify in the research plan section whether or not your application has a health inequalities component or relevance to health inequalities and detail the core set of health inequalities breakdowns that will be reported; if none please explain why. We understand that research projects have different methodologies and focus on different populations, so please explain what data will be collected and reported for the methodology you plan to use. If a health inequalities component is not included, please explain why this does not fit within your proposed research. This should only be a few sentences.
For quantitative research we would ideally like researchers to provide one-way breakdowns of their main outcome(s) by the following equity-relevant variables: age, sex, gender, disability, region, 5 ONS Ethnic groups, and the 5 IMD quintile groups. If more detailed cross tabulations are appropriate, please include these. This table should be submitted to NIHR PRP at the end of the project. Due to data limitations, judgement calls may be necessary about which breakdowns to report and whether to merge categories to increase counts in particular cells; we ask you to make these judgement calls yourself, bearing in mind our data curation aim of enabling future evidence synthesis work in pooling results from different studies. More details and an example table can be found in Appendix A.
For qualitative research projects, this can be purely descriptive statistics giving the number of observations against the various variables.
Further details about this new request can be found in Appendix A.
A recording of the Health Inequalities in NIHR PRP Research Q&A Event which was held on 19 September 2022 is available to view on Youtube.
Areas out of scope for this programme of work
Only NHS regions with ER services should be included in this research.
Other projects e.g., the Offender Personality Disorder pathway. Such projects may engage with the same cohorts, but this research should focus on the ER and any effects that can be attributed to the service.
Technical requirements / Expertise required
We expect a qualitative approach will be best suited to this research as the number of offenders is expected to be quite low.
The ability to co-design research with relevant stakeholders including those with lived experience of complex health needs.
Subject matter expertise on offender health and complex health needs is essential including an in-depth knowledge of the complex needs and barriers faced by these individuals.
Experience with appropriate framing of research findings concerning offender health, high-risk individuals and complex health needs to mitigate further risk of stigmatisation and marginalisation.
Evidence of how previous work has impacted policy and service development, and what role they played in enabling impact.
Outputs
Applicants are asked to consider the timing and nature of deliverables in their proposals. Policymakers will need research evidence to meet key policy decisions and timescales, so resource needs to be flexible to meet these needs. The evaluation of the ER service will provide a formative assessment enabling findings to feed into mobilisation and iterative development of the ER pilot sites. A meeting to discuss policy needs with DHSC officials will be convened as a matter of priority following contracting.
We would like the ER evaluation to begin by January 2024 and an interim report provided in June 2024. The proposed evaluation of ER and mobilisation of the pilot services will happen in parallel. An interim report will inform possible amendments to policy and service specifications and also inform future funding decisions.
It is important that we learn as we mobilise the ER service pilots and act quickly to ensure that any gaps in the service are rectified and that we are giving those who are identified as high risk and have complex needs the best chance to maintain and safeguard their health upon release.
We would like the data to be presented in a variety of different ways such as slide packs and easy-read versions.
Budget and duration
Applications will be assessed on value for money, we would not expect them to cost more than £400K.
The duration of the project should be as short as is consistent with delivering a high-quality study. In order to maximise the benefit from the findings, the research will need to commence as soon as possible following selection of the successful proposals and placing of contracts. Capability to start promptly will be an advantage and for this commissioning round, applicants should demonstrate that studies can start by the relevant date.
Costings can include up to 100% full economic costing (FEC) but should exclude output VAT. Applicants are advised that value for money is one of the key criteria that peer reviewers and commissioning panel members will assess applications against.
Management arrangements
The successful applicants are expected to establish a research advisory group to include, but not limited to, representatives of DHSC, policy colleagues and analytical colleagues from NHS England. The advisory group will meet regularly over the lifetime of the research project and will review the research objectives, provide guidance as well providing opportunity to disseminate emerging findings with stakeholders. They will be expected to:
-
Work with NHSE analysts to gain access to existing datasets relevant to the Enhanced RECONNECT programme
-
Provide regular feedback on progress
-
Produce timely reports to the advisory group
-
Produce a final report for sign off
Research contractors will be expected to work with nominated officials in DHSC, its partners and the NIHR. Key documents including, for example, research protocols, research instruments, reports and publications must be provided to DHSC in draft form allowing sufficient time for review.
NHSE would like a workshop to be held with the ER commissioners to make them aware of the research.
References and key documents
References
- Office of the Deputy Prime Minister (2002) Reducing re-offending by ex-prisoners [Accessed November 2022]
- HM Government (2021) From harm to hope: a 10-year drugs plan to cut crime and save lives [Accessed November 2022]
- HM Government (2021) Preventing suicide in England: Fifth progress report of the cross-government outcomes strategy to save lives [Accessed November 2022]
Key Documents
- HM Government (2018) CONTEST The United Kingdom's Strategy for Countering Terrorism [Accessed November 2022]
- HM Government (2021) £148 million to cut drugs crime [Accessed November 2022]
Appendix A: Further Detail on the New Guidance on Health Inequalities data collection within NIHR PRP Research:
Health Inequalities is a high priority area within the Department of Health and Social Care and the NIHR and is often present in a majority of funded projects. We are now assessing all NIHR research proposals in relation to health inequalities. We are asking applicants to identify in their application whether or not there is a health inequalities component or theme and how this research hopes to impact health inequalities. We are also asking researchers to collect relevant data related to health inequalities, if appropriate for the research. Collecting specific information about health inequalities in research submitted to the programme will allow for categorisation of health inequalities research, curation of data to aid future health inequalities research and enable policymakers to better understand the implications of health inequalities within their policy areas. This is a new request from the NIHR PRP and we will be continuing to monitor queries and adapt the process as needed. If you have any feedback on this new request, please contact us at prp@nihr.ac.uk.
Our goal is to facilitate more widespread and consistent reporting of health inequality breakdown data relating to the primary outcomes of NIHR funded research. We would ideally like researchers to focus on the following equity-relevant variables: age, sex, gender, disability, region*, 5 ONS Ethnic groups**, and the 5 IMD quintile groups. These variables are considered an ideal, but we understand that these are subject to change depending on the sample population and specific research question.
For qualitative research projects, this can be purely baseline characteristics of the participants, for example, the number of participants in each ethnic group.
For quantitative research projects, if there are multiple outcomes/effects with your stakeholders, select a small number of main outcomes as appropriate to report equity breakdowns. We will not be prescriptive about the number of the outcomes, as it will depend on the number of study design types and the nature of the project aims. We are asking for one way cross tabulations of each primary outcome by these equity-relevant variables, if appropriate for your research, together with the number of observations in each cell. If more detailed cross tabulations are appropriate for your proposed research, please include these as well. This request applies to both primary data collection studies and secondary analysis of routine data, and to causal inference studies as well as descriptive studies; however, if this is not possible due to data limitations then please explain. Due to sample size and other data limitations there may be difficult scientific and/or data security*** judgement calls to make about which breakdowns to report and whether to merge categories to increase counts in particular cells; we ask you to make these judgments yourself, bearing in mind our data curation aim of enabling future evidence synthesis work in pooling results from different studies. We also ask that researchers report breakdowns for the unadjusted as well as adjusted outcomes/effects, as appropriate.
We understand that research projects may employ different methodologies, and focus on different populations. Please explain how the variables and data collection methods chosen are appropriate to the methodologies used.
We ask that you please clearly identify in the research plan section of the application whether your application has a health inequalities component or not and detail the core set of health inequality breakdown data that will be collected, if applicable. Submission of the data collection will be a condition of the final report for all research with relevant methodologies regardless of whether the research has a health inequalities component that will need to be submitted to NIHR PRP when the grant has finished. This should only take a few sentences within the research plan section.
* Table below uses the nine regions in England, further regions can be used if using the UK as the study population. Please report region breakdown for large samples in nationally representative descriptive studies. There is no need to report this for small sample studies, for sub-national studies, or for quasi-experimental studies where it would require time-consuming re-estimation.
** White, Mixed/ Multiple ethnic groups, Asian/ Asian British, Black/ African/ Caribbean/ Black British, Other ethnic group. If the sample size is small then it is fine to report only some of the requested equity breakdowns and to merge some of the sub-groups as appropriate.
*** For guidance on how to handle data security concerns in reporting of sensitive data please see ONS guidance.
Example data table for submission at the end of the funded research project
(N.B. If there is more than one main outcome then you will require more tables and if you adjust your outcome then you will need two tables for the adjusted outcome and unadjusted outcome. For other methodologies, variable vs number of observations may be more appropriate to record participant data). This table is for an example only. It does not contain sub variables and does not illustrate any preference for certain variables, as these will be dependent on the proposed research.
| Variable | Outcome (an appropriate average for this subgroup, usually the mean) | Number of observations | Additional information about variation if appropriate, e.g. range, standard deviation |
|---|---|---|---|
| Age | - | - | - |
| Sex | - | - | - |
| Gender | - | - | - |
| Disability | - | - | - |
| Ethnic Group | - | - | - |
| IMD Group | - | - | - |
| Region | - | - | - |
Appendix B: Enhanced RECONNECT priority groups
Priority Group 1: National Security Division (NSD)
- Registered critical public protection cases including sexual or violent offenders who are high profile and of national interest
- Those convicted under the Terrorism Act or where the court states the offence is terrorist connected
- Terrorist risk Service Users (not TACT convicted) who present a national security threat
- All to be assessed
Priority Group 2: At Risk of Extremism (Not NSD)
- Identified as having extremist vulnerabilities
- Channel panel referrals, which includes individuals who are identified as being at risk of being drawn into terrorism.
- All to be assessed
Priority Group 3: Regional Probation Service
- Identified very high/high risk and complex.
The ER cohort will be identified through various national registers of high-risk offenders such as:
- offenders under the Multi-Agency Public Protection Arrangements (“MAPPA”) scheme, which includes offenders who may be liable to management under MAPPA as a consequence of their caution or conviction and sentence and,
- nDelius, a national probation case management system.
Appendix C: Enhanced RECONNECT ‘Team Around Individual’ Model (TAIM)
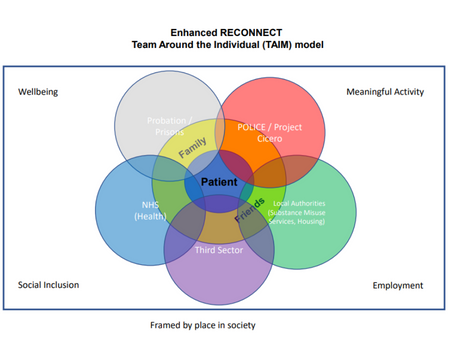
Enhanced RECONNECT Team Around the Individual (TAIM) model
- Well-being
- Social Inclusion
- Meaningful Activity
- Employment
- Probation/Prisons
- POLICE/Project Cicero
- Local Authorities
- Third Sector
- NHS
- Patient
- Family
- Friends
The Team Around Individual Model (TAIM) is akin to a social ecological framework. It places the individual at the centre, whilst recognising available supports, their collaborative working and their proximity to the individual.
Family and Friends occupy the first circle immediately surrounding the individual. Probation/Prisons, POLICE/Project Cicero, Local Authorities (for example, substance misuse services and housing), the Third Sector and the NHS occupy outer circles and all surround patients, and their family and friends.
Wellbeing, Meaningful Activity, Employment and Social Inclusion are the four pillars of the TAIM and areas where Family, Friends, Probation/Prisons, POLICE/Project Cicero, Local Authorities, the Third Sector and the NHS are expected to be able to support the individual.
The TAIM is framed overall by the individual’s place in society.
The ER service will work in a Team Around the Individual Model (TAIM):
The TAIM will consist of a multidisciplinary team that wrap support around the individual. The individual will be an integral part of the team. The basis of all support provided by the ER service will be formulated through the multiagency/disciplinary TAIM meetings. These meetings will be held to support the individual, to ensure that appropriate risk management is in place as identified in the risk assessment and formulated care plan. The TAIM core meeting will be held once a referral has been accepted and the individual assessed by the ER service.
Appendix D: Enhanced RECONNECT Pilot site outcomes and outcomes for individuals
For the pilot areas the high-level outcomes are identified as:
- Improved partnership risk management and safeguarding of the public. This can be measured through case snapshots and discussions with the staff working in the ER service.
- Reduction in repeat offending and risk of harm to self and / or others and a reduction in self-inflicted death. This could be measured through the OASys risk score assessments which are conducted in prisons by HMPPS staff. OASys is an actuarial risk and needs assessment tool used by the prison and probation services in England and Wales. The risk score is based on perceptions of staff and a scoring key is used for this.
- Increased numbers of service users with ongoing substance misuse needs engaging in community substance misuse treatment services within 3 weeks of release.
- Reduction in health inequalities through improved and supported engagement with community health-based services. We only expect the engagement to be measured in line with the previous outcome.
- Consistency in care planning and case management across organisations. This can be measured through case snapshots and discussions with the staff working in the ER service.
Outcomes for individuals
- Improvement in relationships with professionals.
- Improved engagement with health and justice services.
- Improved social inclusion, increased sense of belonging and life skills.
- Reduction in frequency and severity of high-risk behaviours.
- Reduction in health-related re-offending behaviours.
- Improved mental and physical wellbeing.
- Consistency in care planning and case management across organisations pre-release and up to one-year post-release.
- Improved emotional awareness.
Appendix E: Complex Health need description
Complex health needs can be described as having a number of comorbidities which affect an individuals’ quality of life. Also, there is a relationship between someone's physical and mental health. For example, a service user may have lifelong patterns in neglecting their health needs. They may have substance misuse difficulties which impact on their ability to look after their health but have the function of blocking painful memories of flashbacks and nightmares linked to their mental health. They skip meals and eat sugary foods to keep up energy which may make it difficult to manage diabetes or hypertension. Underlying their substance misuse may be problems with pain and they have learnt to switch those feelings off through dependence on certain medications. Also, they neglect their health needs so have poor oral hygiene which causes additional problems with pain.
Appendix F: Further information regarding the RECONNECT Programme
Taken from - NHS commissioning » RECONNECT
RECONNECT is a care after custody service that seeks to improve the continuity of care of vulnerable people leaving prison or an immigration removal centre (IRC). This involves working with them before they leave to support their transition to community-based services, thereby safeguarding health gains made whilst in prison or an IRC.
RECONNECT services aim to improve the wellbeing of people leaving prison or an IRC, reduce inequalities and address health-related drivers of offending behaviours. Whilst not a clinical service, RECONNECT offers liaison, advocacy, signposting, and support to facilitate engagement with community- based health and support services.
RECONNECT services also aim to:
- Increase access to and uptake up of healthcare or relevant support services for individuals who have health vulnerabilities* upon release from prison or IRCs who would otherwise struggle to engage
- Ensure that the health needs of individuals who are leaving prison or IRCs are met
- Ensure a safe transition from prison or IRC to community-based healthcare and support services in England
- Provide follow-up to ensure engagement is maintained
Who is RECONNECT for?
Any person aged 18 or above leaving a secure or detained setting (prison or IRC) with an identified health vulnerability which means that they would otherwise struggle to engage with community-based healthcare services and / or relevant support services.
What will RECONNECT do?
- Offer support and release planning to individuals for up to 12 weeks prior to release or as soon as they are referred within the 12 weeks prior to their release.
- Offer support for up to 6 months post-release date, or when all health care needs are met – whichever comes soonest (this may be extended in exceptional circumstances when it would be detrimental to the health of the individual to be discharged at 6 months).
- Undertake an assessment of appropriateness of the referral and gain patient consent.
- Offer the patient a minimum of 2 points of face-to-face contact prior to their release. If it is not possible to do face to face, then virtual, telephone or a combination of these methods will be offered.
- Provide individuals with a named RECONNECT member of staff who will work with them prior to, and upon release, until they are engaged with an appropriate community-based health service care or support service appointment or are discharged from the service. Peer support should be available for every prison leaver where appropriate.
- Work in a trauma informed way.
- Ensure that where the individual is being held in an establishment outside of their home area, the RECONNECT service local to the prison and / or IRC will facilitate communication between the prison / IRC, the individual and receiving RECONNECT service.
- Work closely with prison and / or IRC based healthcare teams, including physical and mental health services, substance misuse services and relevant support services.
- Offer a holistic service that meets the needs of the individual.
- Support those on Release on Temporary Licences (ROTL) up to 12 weeks before final release date where appropriate.
How can I access RECONNECT?
RECONNECT operates on a referral system. Referrals can be accepted from probation services, police, Liaison and Diversion services and / or Home Office enforcement teams for individuals who have been released in the past 28 days.
Self-referrals and those from friends and family can be made on behalf of an individual whilst they are in prison or immigration removal centre. We recommend they discuss this with their prison healthcare team or probation officer who can advise them how to refer to their local RECONNECT service.